1/7
LEFT OR RIGHT?
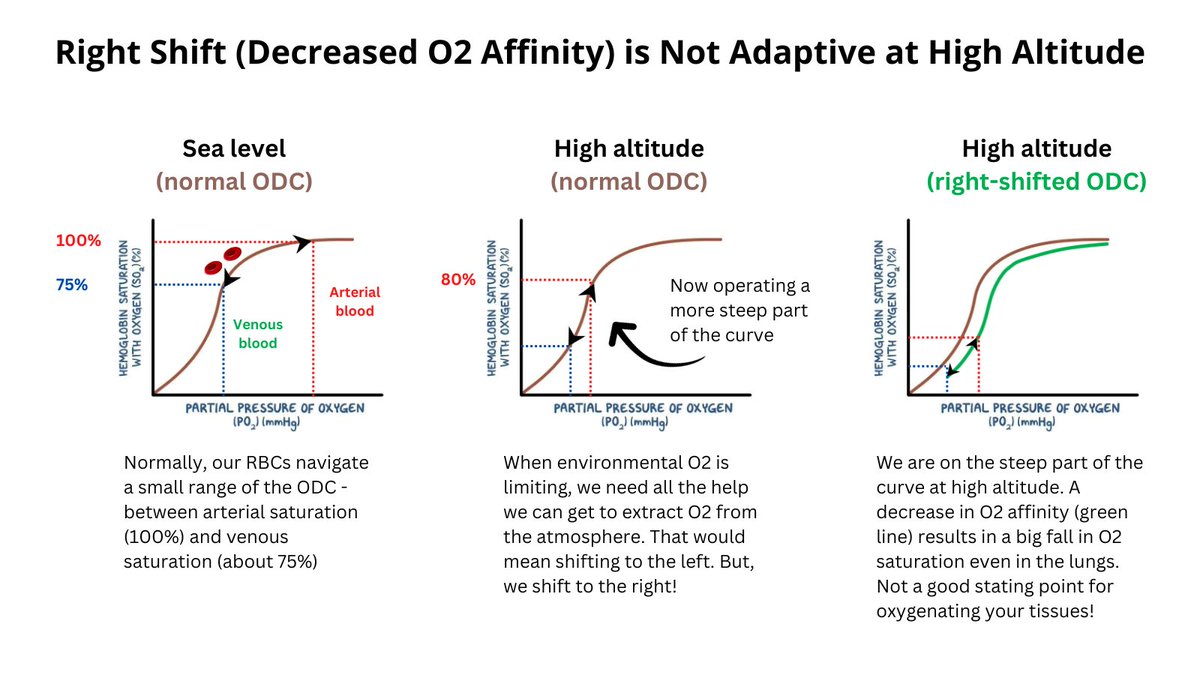
I recently tweeted asking whether the rightward shift of our O2 dissociation curve (ODC) (reduced O2 affinity, increased O2 offloading in tissues) when we climb a mountain is a good thing.
LEFT OR RIGHT?
I recently tweeted asking whether the rightward shift of our O2 dissociation curve (ODC) (reduced O2 affinity, increased O2 offloading in tissues) when we climb a mountain is a good thing.

2/7
I pointed out that animals that have evolved at high altitude (e.g., bar-headed goose, llama) actually shift their curve to the left (they have a special mutation in their Hb).
I pointed out that animals that have evolved at high altitude (e.g., bar-headed goose, llama) actually shift their curve to the left (they have a special mutation in their Hb).
3/7
Similarly, human fetuses, who are normally exposed to limiting amounts of O2 from mom's circulation, shift their ODC to the left (a characteristic feature of fetal Hb).
Similarly, human fetuses, who are normally exposed to limiting amounts of O2 from mom's circulation, shift their ODC to the left (a characteristic feature of fetal Hb).
4/7
To further address the question of whether a left or right shift is adaptive at high altitude, a 1974 paper in Science reported that rats chemically manipulated to shift their ODC to the left fared better when exposed to simulated high altitude.
To further address the question of whether a left or right shift is adaptive at high altitude, a 1974 paper in Science reported that rats chemically manipulated to shift their ODC to the left fared better when exposed to simulated high altitude.

5/7
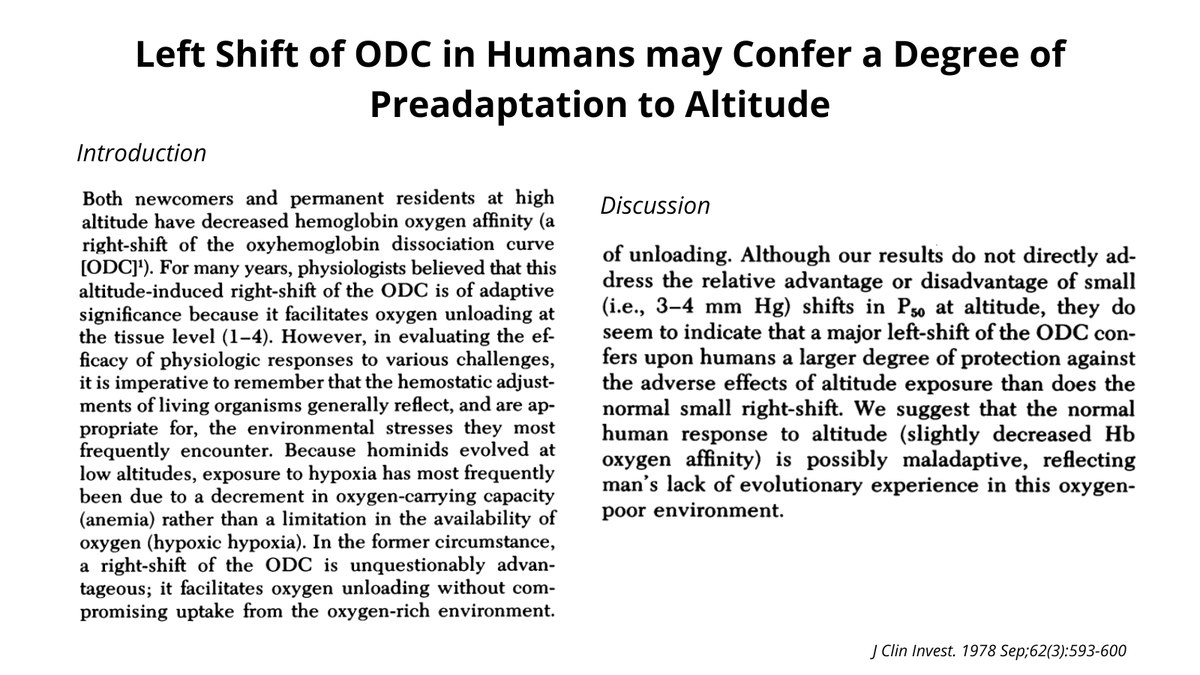
This was followed by a classic study by Bob Hebbel, a hematologist at the University of Minnesota. He reasoned that if a shift to the left is adaptive at high altitude, then humans with congenital high-affinity hemoglobin should do better under these conditions.
This was followed by a classic study by Bob Hebbel, a hematologist at the University of Minnesota. He reasoned that if a shift to the left is adaptive at high altitude, then humans with congenital high-affinity hemoglobin should do better under these conditions.

6/7
Indeed, this is what he found. He took 2 subjects with Hb Andrew-Minneapolis and 2 of their normal siblings up to about 9,000 ft. for 10 days and showed that the ones with Hbopathy fared better.
Such a cool experiment that would NEVER be funded in this era!
Indeed, this is what he found. He took 2 subjects with Hb Andrew-Minneapolis and 2 of their normal siblings up to about 9,000 ft. for 10 days and showed that the ones with Hbopathy fared better.
Such a cool experiment that would NEVER be funded in this era!
7/7
The bottom line then is that in situations where environmental oxygen is limiting (high altitude, in the womb), the benefit of increasing O2 uptake in lungs/fetus with a shift to the left outweighs the disadvantage of unloading less O2 to the tissues.
The bottom line then is that in situations where environmental oxygen is limiting (high altitude, in the womb), the benefit of increasing O2 uptake in lungs/fetus with a shift to the left outweighs the disadvantage of unloading less O2 to the tissues.
• • •
Missing some Tweet in this thread? You can try to
force a refresh