Here's a great roundup on what the Long COVID Community has learned from recent clinical trials, from the always insightful @CortJohnson Definitely worth a read! 🤔🧠
Cort draws several key points from these trials, including:
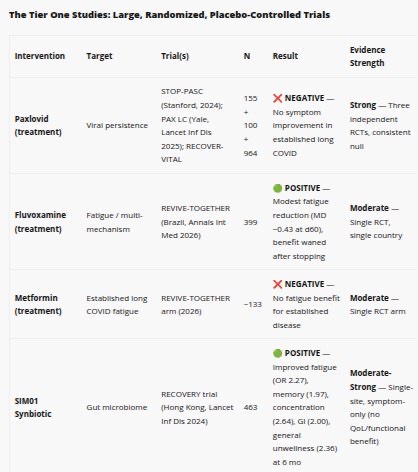
👉Short term antiviral treatments don't work. It's somewhat surprising after we've all heard the anecdotes of some patients improving on 5-10 days of Paxlovid. Unfortunately, trial results do not show a benefit here.
👉Treatments that prevent Long COVID don't necessarily work to treat it - as in the case of Metformin
👉Interestingly, the reverse is true. Treatments that don't prevent Long COVID at all - as in the case of the antidepressant fluvoxamine - actually have been shown to treat it.
👉Narrow treatments are less helpful than broadly acting ones. For example, Paxlovid has been proven to be less helpful in preventing Long COVID than metformin. Paxlovid ONLY targets SARS-CoV-2 replication, whereas metformin is a host-directed antiviral that affects multiple bodily systems.
There's a lot more great info here - highly recommend checking out the article!
1/
Cort draws several key points from these trials, including:
👉Short term antiviral treatments don't work. It's somewhat surprising after we've all heard the anecdotes of some patients improving on 5-10 days of Paxlovid. Unfortunately, trial results do not show a benefit here.
👉Treatments that prevent Long COVID don't necessarily work to treat it - as in the case of Metformin
👉Interestingly, the reverse is true. Treatments that don't prevent Long COVID at all - as in the case of the antidepressant fluvoxamine - actually have been shown to treat it.
👉Narrow treatments are less helpful than broadly acting ones. For example, Paxlovid has been proven to be less helpful in preventing Long COVID than metformin. Paxlovid ONLY targets SARS-CoV-2 replication, whereas metformin is a host-directed antiviral that affects multiple bodily systems.
There's a lot more great info here - highly recommend checking out the article!
1/
@CortJohnson Link: healthrising.org/blog/2026/04/2…
• • •
Missing some Tweet in this thread? You can try to
force a refresh







