
Flu pandemics recur reliably but unpredictably every decade or so, and their extent and intensity varies. With COVID19, we may be in midst of a once-every-50-years event, perhaps similar to 1957 pandemic, but not as bad as the 1918 pandemic. Let’s talk about the 1957 pandemic. 1/
Pandemics result from emergence of viral strains that are novel, often from genetic recombination in animal reservoirs. The 1957 pandemic was due to influenza A (H2N2). cdc.gov/flu/about/viru… "Serological archeology" suggests it resembled 1889 strain. ncbi.nlm.nih.gov/pubmed/8877331 2/
The virus that caused the 1957 pandemic is a different from the coronavirus causing COVID19. Both are rhinoviruses, but from different phyla. statnews.com/2020/03/03/who… Despite the different pathogens, we can still understand what is happening by studying past pandemics. 3/
First, here is a timeline via our amazing @CDCgov of the history of public health responses to flu pandemics: cdc.gov/flu/pandemic-r… 4/
Best estimate at present is COVID-19 has intermediate transmissibility compared to other pandemics (an effective reproductive rate, Re, of 2-4 new cases per old case) & intermediate mortality (0.5%-2.0%, though still unclear). This makes it serious. ncbi.nlm.nih.gov/pmc/articles/P… 5/
A classic 1961 paper analyzing the 1957 pandemic ncbi.nlm.nih.gov/pubmed/13758900 concluded that the disease likely started in central China (like COVID-19) and became known to the rest of the world in April of 1957. Pandemics have started in many continents. 6/
Globally, the 1957 pandemic killed 1.1M people. There was regional variation; for instance: 0.3 deaths/10,000 in Egypt and 9.8/10,000 in Chile. GDP and latitude explained 43% of the variance in excess mortality. ncbi.nlm.nih.gov/pmc/articles/P… 7/
Mortality in the 1957 global flu pandemic was U-shaped, with the very young and very old dying (ncbi.nlm.nih.gov/pubmed/8877331). This is typical, but this appears NOT to be the case with COVID-19, where the young are spared (medrxiv.org/content/10.110… ). 8/
The first wide awareness of the 1957 pandemic in the USA was a tiny article on April 17, 1957 in the @nytimes on page 3 noting that 250,000 people were afflicted in Hong Kong (or 10% of the population). 9/
The 1957 pandemic was first recognized in USA in June in RI, but other outbreaks soon occurred in CA. By September, it was everywhere. And it recurred when schools re-opened in fall of 1957. A first peak in excess death was in October, and a second peak in February of 1958. 10/
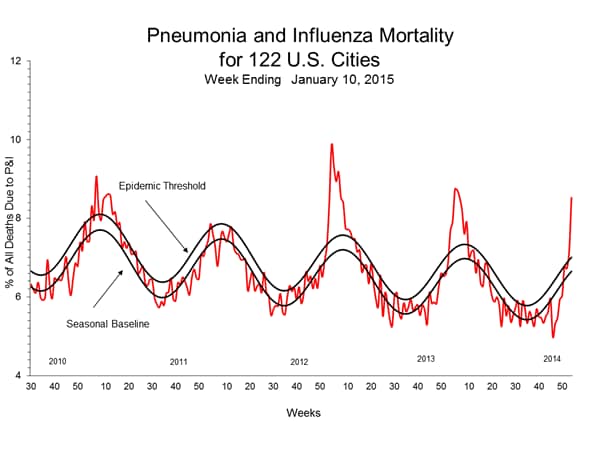
Peaks in epidemics have to do with: pathogen flows across networks; other social factors (like changes in population mixing across time, or school re-openings); weather; etc.. For instance, flu has a baseline seasonality. cdc.gov/flu/weekly/wee… 11/
{kind=link}
Here is a focused image of waves of the 1957 flu, in a relatively mildly affected area in Arizona. The waves are apparent, as the flu comes and goes. bmcinfectdis.biomedcentral.com/articles/10.11… 12/
Ultimately, 115,700 excess deaths occurred in the USA from the 1957 flu pandemic (pop size was 172 million, and cancer killed 255,000 people that year). It was a leading killer (and many experts now fear COVID19 might be -- though we still don't know). cdc.gov/nchs/data/vsus… 13/
The 1957 pandemic tended to attack young people more, according to focused contemporaneous studies in LA and MO (which is why, incidentally school closures are so effective at retarding spread), but mortality was highest in the very long and very old, in an inverted U shape. 14/
Pertinently, NOT everyone was afflicted in 1957, however. The overall attack rate was 41% in LA & 34% in MO. For COVID19, experts like @mlipsitch estimate that 20-60% of people will ultimately contract the pathogen. This is typical of flu epidemics. ncbi.nlm.nih.gov/pubmed/8877331 15/
But mortality from 1957 outbreak in the USA was U-shaped, as most pandemics are, killing the very young (<5) and very old (>65). ncbi.nlm.nih.gov/pubmed/8877331/ This is different than COVID19, which seems to spare the young (like some other flus) (medrxiv.org/content/10.110…). 16/
This combination of facts (school-aged people attacked, young & old die) reflects general pattern whereby the virus spreads in people who are out & about (at school & work) interacting. Virus is ‘brought home’ to kill age extremes who are at the end of the transmission chain. 17/
Therefore, immunizing the old, while it will reduce deaths, does not have much effect on the actual course of the epidemic. Everyone has to be immunized to get herd immunity, and immunizing working-age people helps break chains of transmission through social networks. 18/
The 1957 pandemic ended as people became immune over a period of three years. Possibly the virus became less virulent too. We can expect COVID19 to similarly become 'endemic,' but probably after several waves of affliction, alas. ncbi.nlm.nih.gov/pmc/articles/P… 19/
In the modern era, we control pandemics by surveillance (and testing!) and rapid development of vaccines (but even “rapid” development is 12-18 months, alas). 20/
In sum, COVID-19 resembles 1957 influenza pandemic in certain epidemiological ways (despite different pathogen & different age curve), which is what makes it more alarming than other pandemics that periodically afflict us. We're still not certain, but will know more soon. 21/
#3 in this thread involved an infuriating autocorrect error! This should read RIBOVIRUS, not rhinovirus. Both COVID-19 and 1957 flue are riboviruses. Influenza A is Riboviria, Phylum: Negarnaviricota, and Coronavirus is Riboviria, Phylum: incertae sedis. 22/
I'd like to update my assessment, from exactly 3 months ago, re the likely severity of the COVID-19 pandemic, using a classic schema (wwwnc.cdc.gov/eid/article/19…). I think this pandemic will take at least 300,000 lives in USA, even as many as 500,000, before it's done. It's bad. 23/
Share this Scrolly Tale with your friends.
A Scrolly Tale is a new way to read Twitter threads with a more visually immersive experience.
Discover more beautiful Scrolly Tales like this.