a fresh meta-analysis of steroids shows that they increase GI bleeds! sounds scary, but let's look into this further... (#rantorial 1/7)
https://twitter.com/yourICM/status/1191989062145642497?s=20
the meta-analysis detected a barely significant increase in "clinically significant bleeding" in patients treated with steroid. there was *no* difference in bleeding of any severity. why this discrepancy? let's dig deeper...(2/7)
ncbi.nlm.nih.gov/pubmed/31501997
ncbi.nlm.nih.gov/pubmed/31501997

the primary endpoint ("clinically significant" bleeding) was only reported in 25 trials. most are small. nearly *half* of the power in this analysis comes from a single trial, Roberts 2004... what was going on here? (#rantorial 3/7)
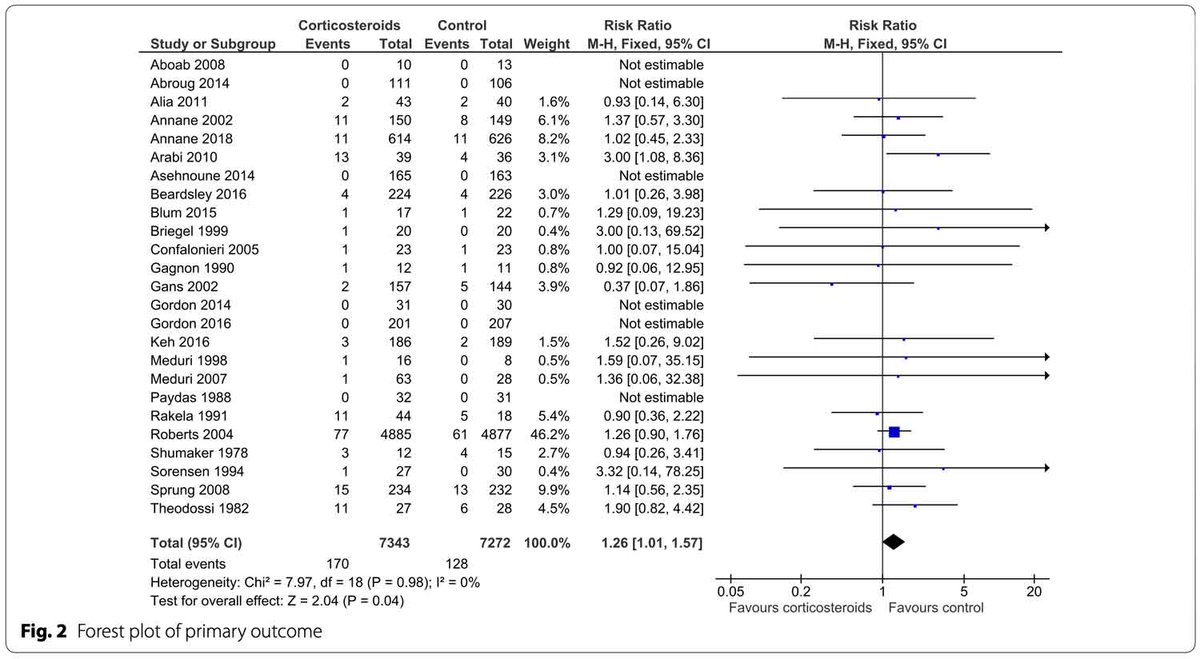
digging into the supplemental data shows that the Roberts 2004 trial involved giving astronomically massive doses of steroid for traumatic brain injury! of course that caused GI bleeding! (#rantorial 4/7)

the primary analysis is missing some major studies (ADRENAL etc). perhaps these studies didn't specifically record "clinically significant" bleeds, so they weren't included. this causes the primary endpoint to be dominated by wierd studies like Roberts 2004 (#rantorial 5/7)
the secondary endpoint, GI bleeding of any severity, included a lot more studies (55 vs. 25). this may explain the discrepancy between the primary endpoint versus the secondary endpoint (which *didn't* find harm from steroid)(#rantorial 6/7)
this study illustrates the a classic pitfall of meta-analyses: blenderizing together profoundly heterogenious studies to achieve a barely significant result (p=0.04) and then suggesting that it means something. (#rantorial 7/7)
• • •
Missing some Tweet in this thread? You can try to
force a refresh