
A thread on our recent analysis of WES, RNAseq, and clinical predictors of response to PD-1 ICB in metastatic melanoma patients led by @vanallenlab, Dirk Schadendorf, and Bastian Schilling with many others!
@NatureMedicine @DanaFarber @broadinstitute
nature.com/articles/s4159…
@NatureMedicine @DanaFarber @broadinstitute
nature.com/articles/s4159…
@VanAllenLab @NatureMedicine @DanaFarber @broadinstitute Our cohort was 144 metastatic melanoma patients who received PD-1 ICB. Overall response rate (CR or PR) was 38%; and subtypes were 86% cutaneous or occult melanoma, 7% acral, and 7% mucosal. Median follow-up was 30 months. 39% had BRAF mutations, 30% NRAS, and 17% NF1. [2/n] 
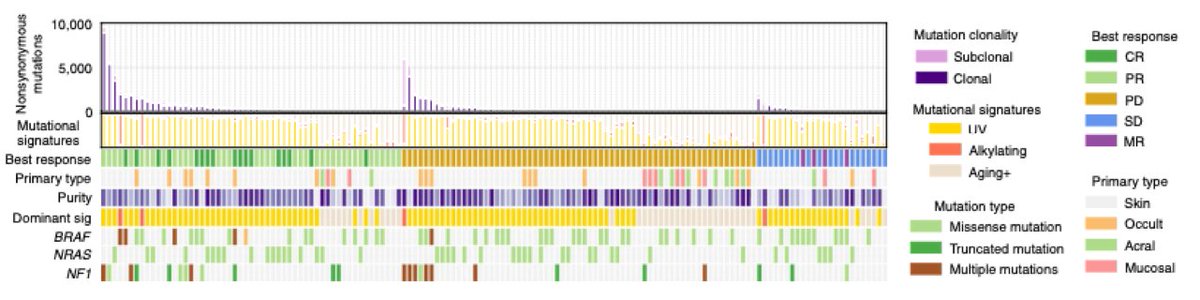
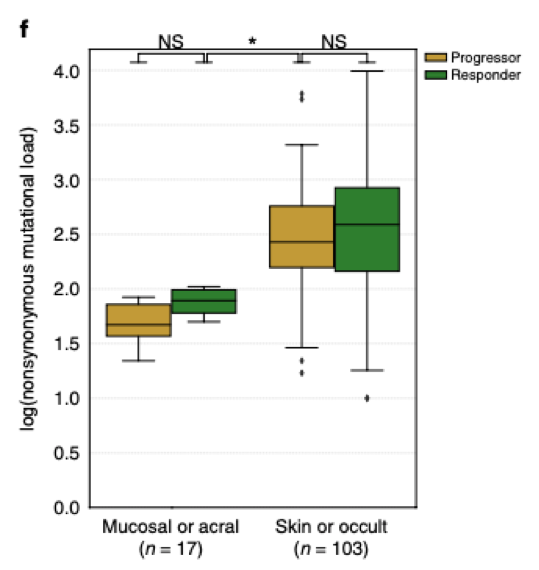
@VanAllenLab @NatureMedicine @DanaFarber @broadinstitute TMB was higher in responders vs. non-responders overall, as seen previously, but the effect is confounded by melanoma subtype; mucosal and acral melanomas have lower TMB and response rates. Stratified by subtype, the difference in TMB is no longer statistically significant. [3/n]
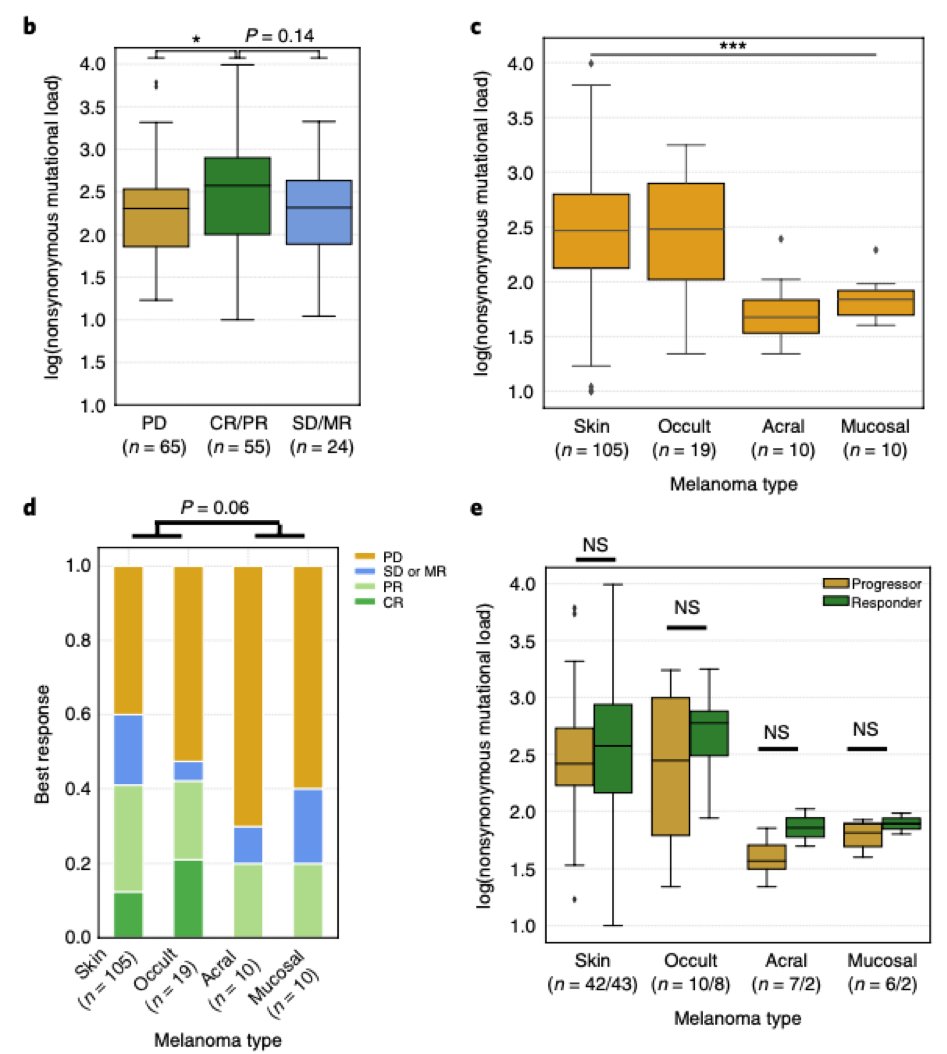
@VanAllenLab @NatureMedicine @DanaFarber @broadinstitute Notably, acral and mucosal responders had lower mutational burden than cutaneous and occult progressors, suggesting that any TMB threshold needs to be considered in the context of melanoma subtype. [4/n]
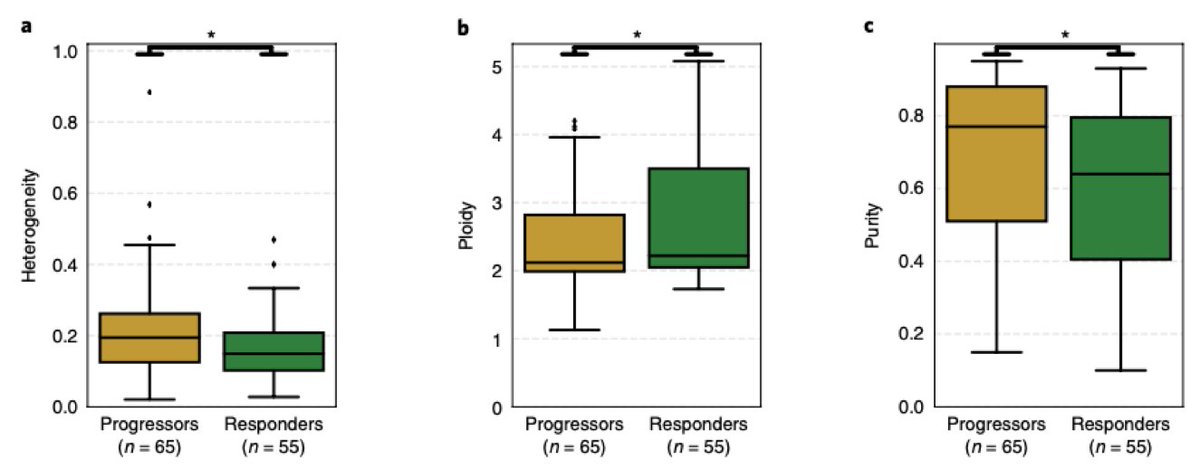
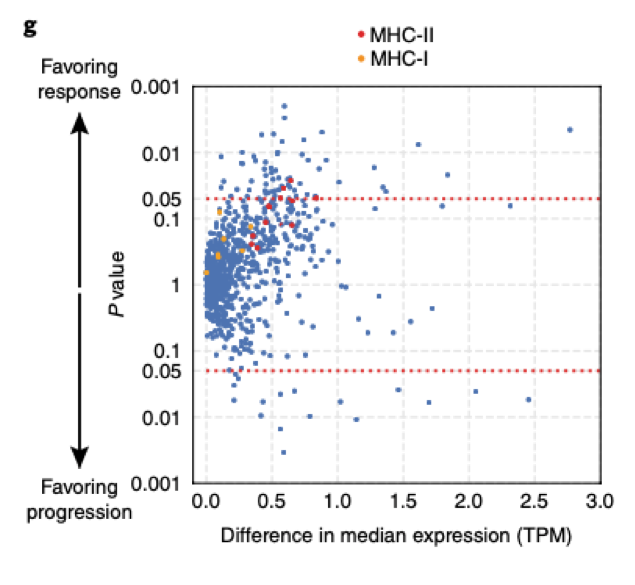
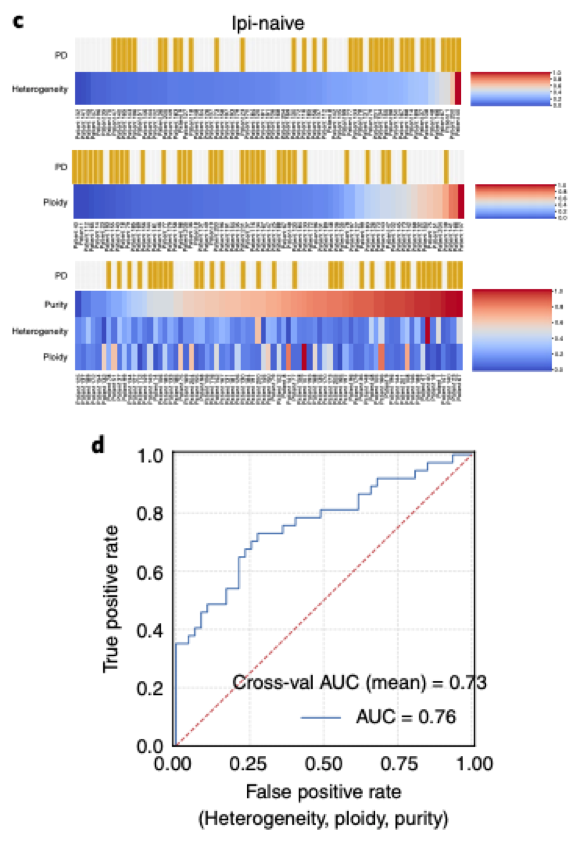
@VanAllenLab @NatureMedicine @DanaFarber @broadinstitute Intratumoral heterogeneity and tumor purity (proportion of tumor cells in the tumor sample) inferred from genomic data was higher in progressors vs responders. Tumor ploidy was lower in progressors. Antigen presentation gene expression was higher in responders [5/n]
@VanAllenLab @NatureMedicine @DanaFarber @broadinstitute 60/144 patients had ipilimumab (anti-CTLA4 ICB) prior to PD-1 ICB, and we hypothesized that predictors of response may differ based on prior therapy (though having similar overall response rates). We subsequently compared ipi-treated vs -naive patients. [6/n]

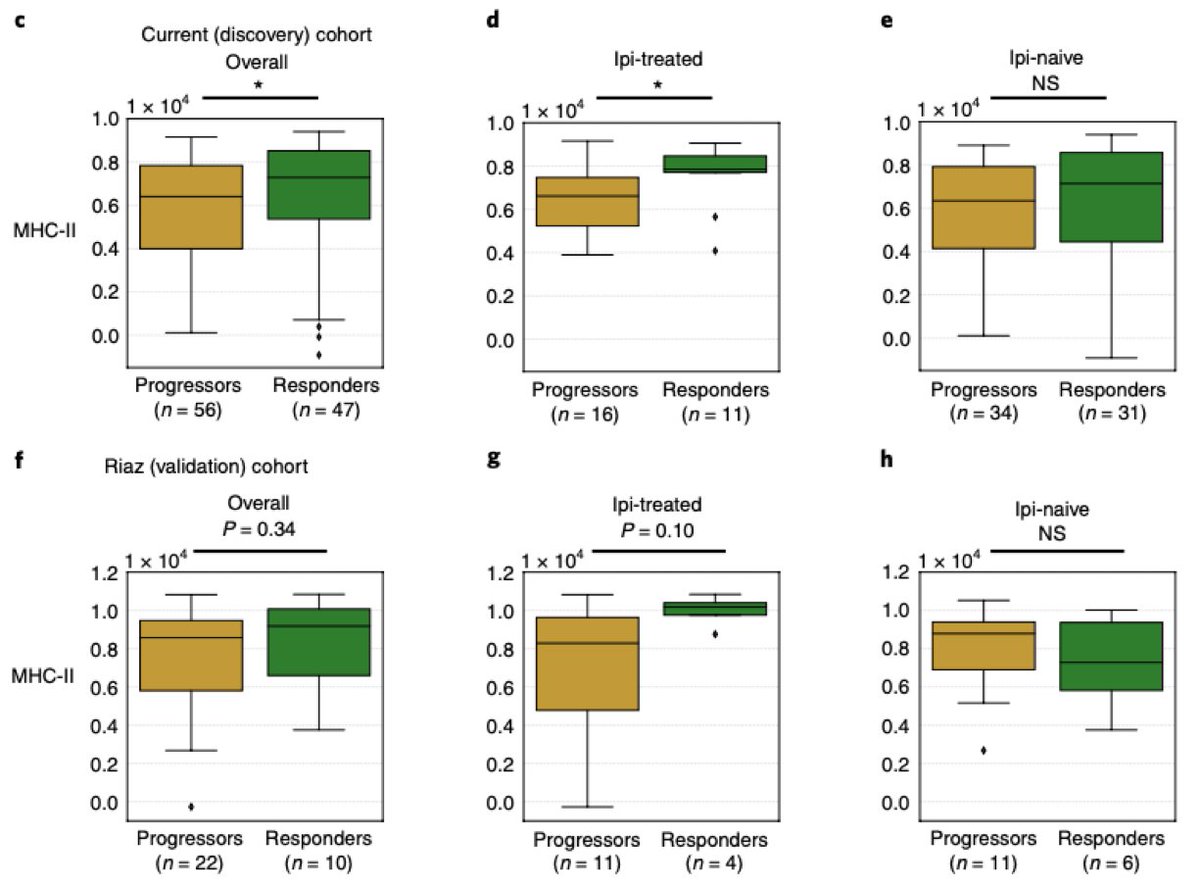
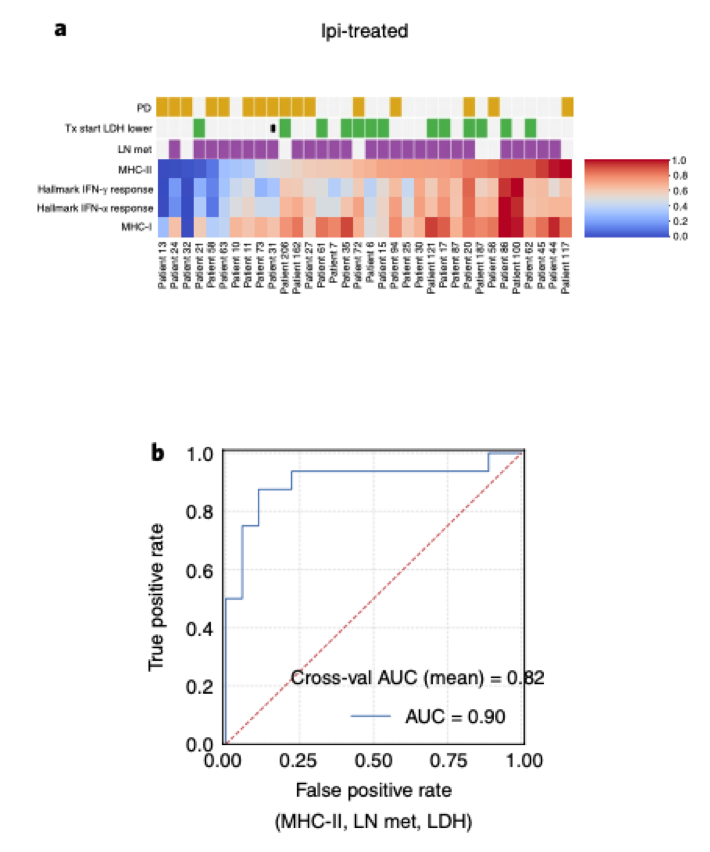
@VanAllenLab @NatureMedicine @DanaFarber @broadinstitute Higher MHC-II expression in responders vs. progressors is found in the ipi-treated but not the -naive subgroup; we find the same relationship in an independent PD-1 ICB treated melanoma cohort (though not statistically significant in this smaller cohort) [7/n]
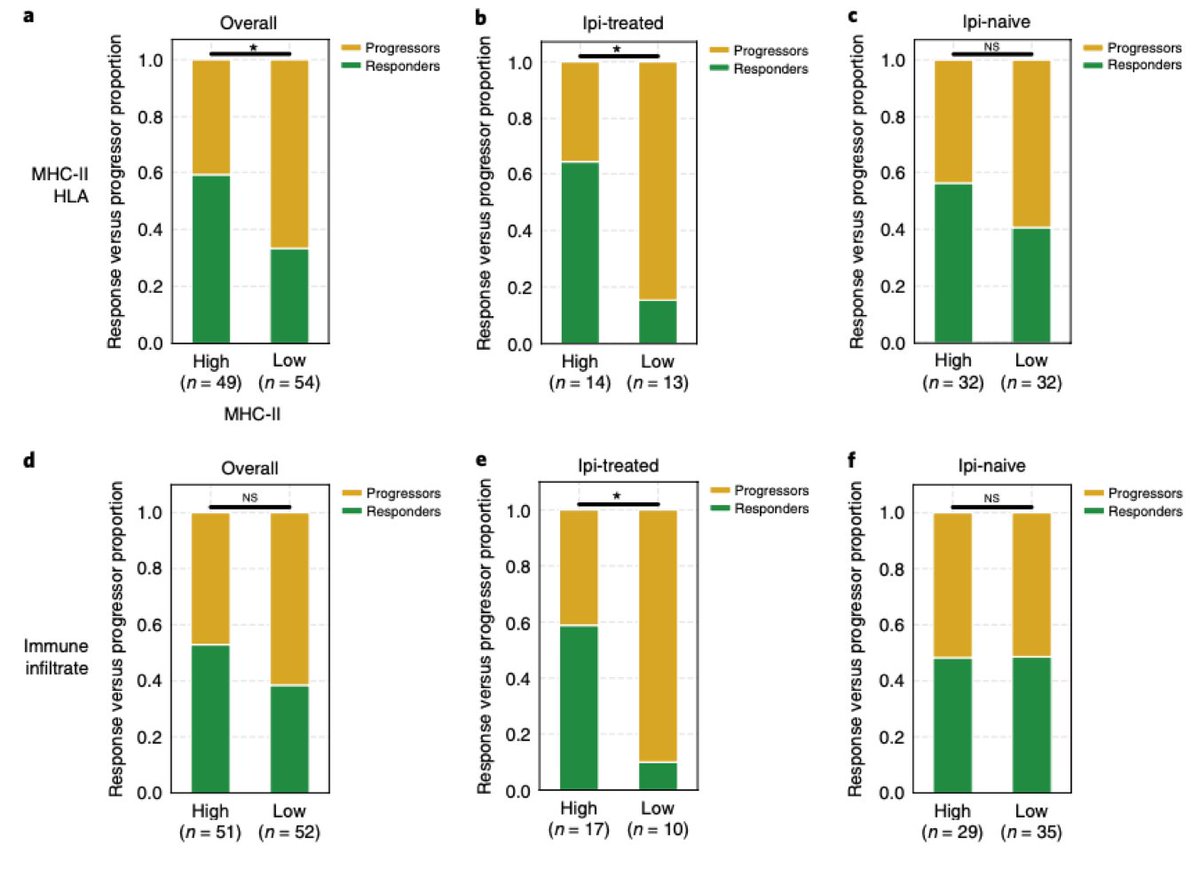
@VanAllenLab @NatureMedicine @DanaFarber @broadinstitute Splitting the overall cohort by high and low MHC-II expression and immune infiltrate, we find that these immune activity markers are excellent predictors only in the ipi-treated subgroup. [8/n]
@VanAllenLab @NatureMedicine @DanaFarber @broadinstitute Leading us to the following proposed model: ipi-treated tumors with low evidence of immune activity post-ipi are highly unlikely to respond to subsequent anti-PD1 ICB, but immune activity in ipi-naive tumors does not predict response [9/n]
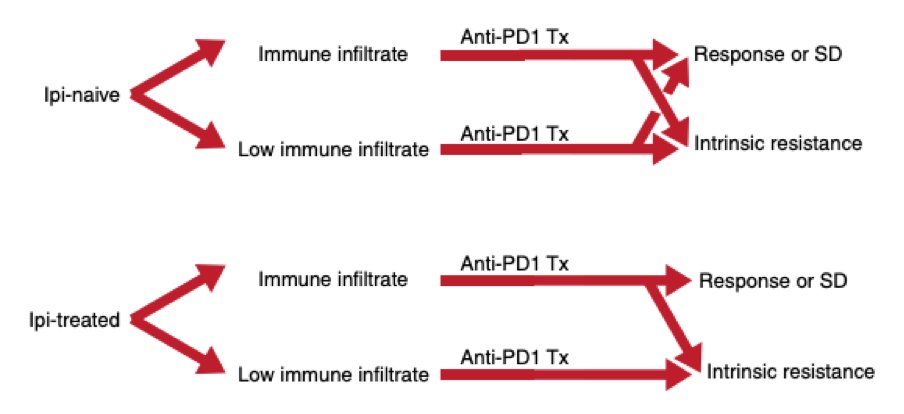
@VanAllenLab @NatureMedicine @DanaFarber @broadinstitute Leading us to the following proposed model: ipi-treated tumors with low evidence of immune activity post-ipi are highly unlikely to respond to subsequent anti-PD1 ICB, but immune activity in ipi-naive tumors does not predict response [9/n]
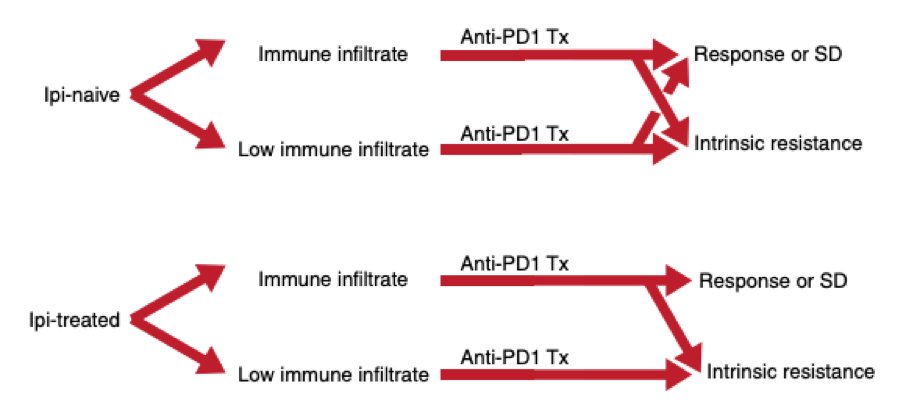
@VanAllenLab @NatureMedicine @DanaFarber @broadinstitute Based on these findings, we built models to predict intrinsic resistance to therapy separately for ipi-naive and -treated tumors, integrating clinical and molecular features. [10/n]
@VanAllenLab @NatureMedicine @DanaFarber @broadinstitute For ipi-treated patients, a model with MHC-II expression, LDH, and lymph node mets had a cross-validation AUC of 0.82 (and AUC of 0.9). [11/n]
@VanAllenLab @NatureMedicine @DanaFarber @broadinstitute For ipi-naive tumors, a model incorporating heterogeneity, ploidy, and purity had a cross-validation AUC of 0.73 and AUC of 0.76. [12/n]
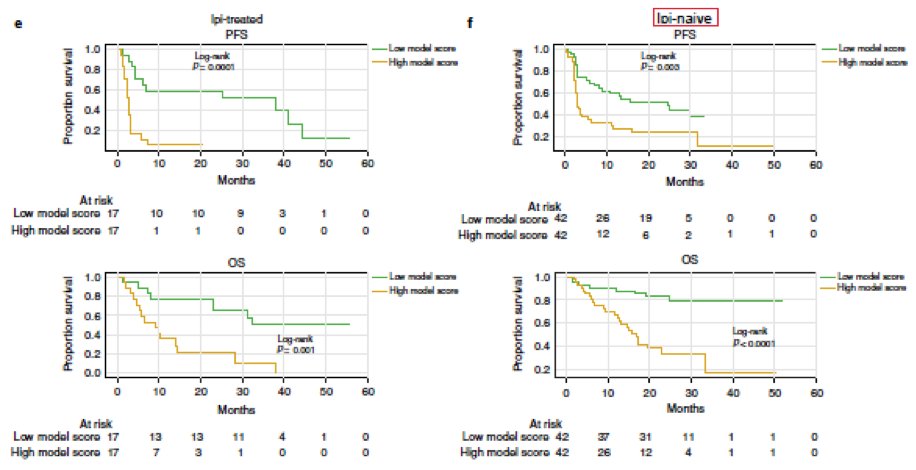
@VanAllenLab @NatureMedicine @DanaFarber @broadinstitute These models were built to predict RECIST response, but also stratified survival nicely [13/n]
@VanAllenLab @NatureMedicine @DanaFarber @broadinstitute Important caveat: We could not find an appropriate validation cohort with all molecular and clinical data (e.g. prior treatment, biopsy time-frame) necessary to independently validate our models. [14/n]
@VanAllenLab @NatureMedicine @DanaFarber @broadinstitute Data for our study is available: processed molecular and clinical data are in the supplements, and raw sequencing data should shortly be available in dbGap. #cancermoonshot [15/n]
@VanAllenLab @NatureMedicine @DanaFarber @broadinstitute There is much work yet to be done to get to clinical predictive models and biomarkers (e.g. standardized model features), but our study highlights the importance of clinical context and integrating clinical and molecular data in building clinically-applicable biomarkers! [16/n]
@VanAllenLab @NatureMedicine @DanaFarber @broadinstitute Thanks to the many, many contributors to this study, from clinical investigators to computational biologists throughout Germany and Europe and the United States, under the supervision of Dirk Schadendorf, Eli Van Allen (@vanallenlab), and co-led by Bastian Schilling. [17/n]
@VanAllenLab @NatureMedicine @DanaFarber @broadinstitute Thanks to our funders, and most of all, heartfelt thanks to our patients who have selflessly contributed so that future patients may benefit! @DanaFarber @UniklinikEssen @broadinstitute @DamonRunyon @NIH @theNCI @dfg_public @sitcancer @conquercancerfd #JMUW [18/n FIN]
@VanAllenLab @NatureMedicine @DanaFarber @broadinstitute @UniklinikEssen @DamonRunyon @NIH @theNCI @dfg_public @sitcancer @ConquerCancerFd My mentor and senior author @vanallenlab with a complementary thread on this work adding context and commentary

