finally read this article on "acute severe hypertension" in NEJM and it's even worse than I was expecting... 🤯 (#rantorial 1/4)
https://twitter.com/dan___kim/status/1207334320760737794?s=20
the NEJM article directly contradicts established guidelines & practice regarding hypertensive urgency (#rantorial 2/4) 

for a review which is consistent with guidelines & not awful, take a look at the @iBookCC chapter (#rantorial 3/4)
emcrit.org/ibcc/hypertens…
emcrit.org/ibcc/hypertens…
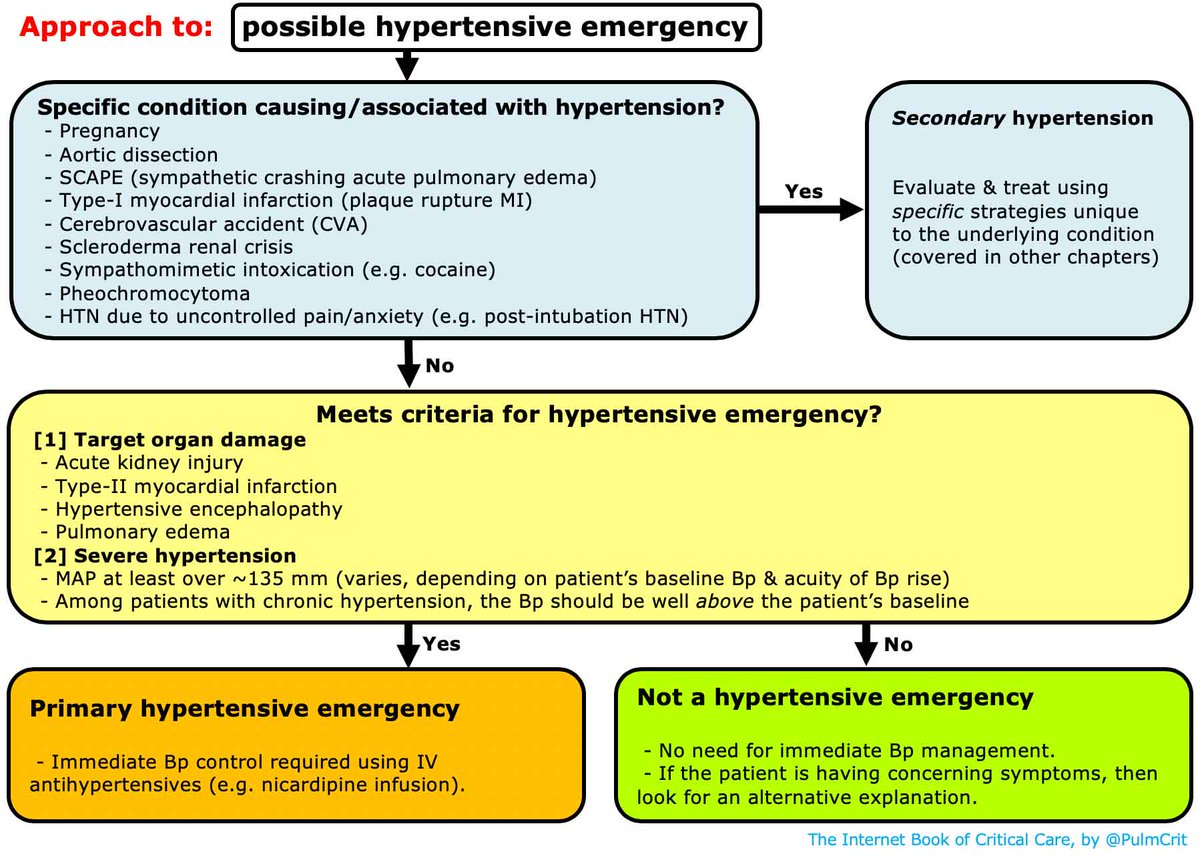
to try to further dispel nonsense about emergent therapy for asymptomatic hypertension, I've added the following figure to the IBCC chapter, with links to the guideline. (#rantorial 4/4)

• • •
Missing some Tweet in this thread? You can try to
force a refresh