
Mumsnet is in financial trouble. According to their CEO its "squeaky bum time".
With less money floating about, advertisers are carrying out more due diligence, I expect those businesses which support anti-LGBT sentiment are more at risk. Mumsnet transphobia was bad business.
With less money floating about, advertisers are carrying out more due diligence, I expect those businesses which support anti-LGBT sentiment are more at risk. Mumsnet transphobia was bad business.
Birdseye money ran out in October 2018 #mumsnettransphobia
https://twitter.com/DadTrans/status/1122121214351290368
Flora used to bear a #mumsnet logo. They severed the relationship following a reasonable question from a mum of a trans teen who didn't want to buy a product associated with a hate forum. #boycottTransphobia #mumsnettransphobia
https://twitter.com/StopFundingHate/status/1182670502353145858
Their CEO has regular fawning articles in the UK press (mainly the Telegraph, one of the most anti trans papers), including sponsored content & authored puff pieces. This doesn't seem to have helped much... 




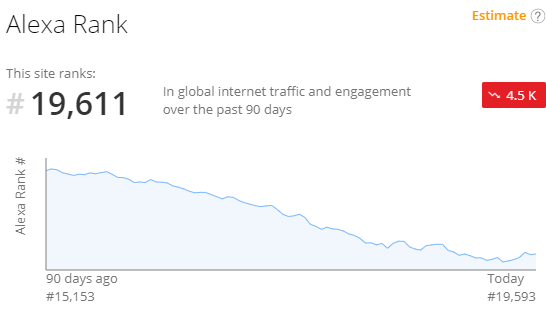
Web traffic to the site has nearly halved in the last 9 months. While their CEO is blaming coronavirus, the rot set in long ago. Little changed since its launch in 2000 the site looks increasingly anachronistic, a relic, surviving as an internet meme.

I expect Justine hasn't kicked off those users spouting transphobic vitriol not because of a commitment to free speech (indeed they've been quick to comply with those slandered threatening legal action) but because they can't afford to lose some of their most active users
I'll end with the below, most forlorn, entry. A survey put out on twitter by @MumsnetTowers just a few weeks ago on the subject of coronoavirus and pregnancy. The account with 153,000 followers attracted a single like, just one retweet- the loan sharer their CEO, Justine Roberts.
Addendum. Mumsnet made £2.245 million profit after tax in 2017 & £2.221 in 2018 (companies house). According to the CEO "last year we made a profit of 570k. This year so far we are loss making". They've taken & extended a loan, staff on reduced hours & a pay holiday for the CEO.


• • •
Missing some Tweet in this thread? You can try to
force a refresh




