NIGHTINGALE REHAB SERVICE
- What could it look like?
- How could it be staffed?
- How could it be implemented?
@MSKReform & partners have been pondering these Qs for the last few weeks so here’s an overview for your consideration! THREAD 1/
Full text: mskreform.org.uk/nightingalereh…
- What could it look like?
- How could it be staffed?
- How could it be implemented?
@MSKReform & partners have been pondering these Qs for the last few weeks so here’s an overview for your consideration! THREAD 1/
Full text: mskreform.org.uk/nightingalereh…

But first, is it required?
@alicecamurray, @ClareGerada & Dr J Morris make the case in this brilliant @HSJnews article: hsj.co.uk/commissioning/…
They also lay out their take on what it could look like, much of which I agree with so we were delighted to read this timely piece! 2/
@alicecamurray, @ClareGerada & Dr J Morris make the case in this brilliant @HSJnews article: hsj.co.uk/commissioning/…
They also lay out their take on what it could look like, much of which I agree with so we were delighted to read this timely piece! 2/
On implementation, I suggest a national framework which includes a best-practice operating model & clinical competencies which focus on the principles of quality functional rehabilitation.
REHAB IS A GREAT UNIFIER (as was proposed in policy Ex3 of the @MSKReform manifesto 😉) 3/
REHAB IS A GREAT UNIFIER (as was proposed in policy Ex3 of the @MSKReform manifesto 😉) 3/
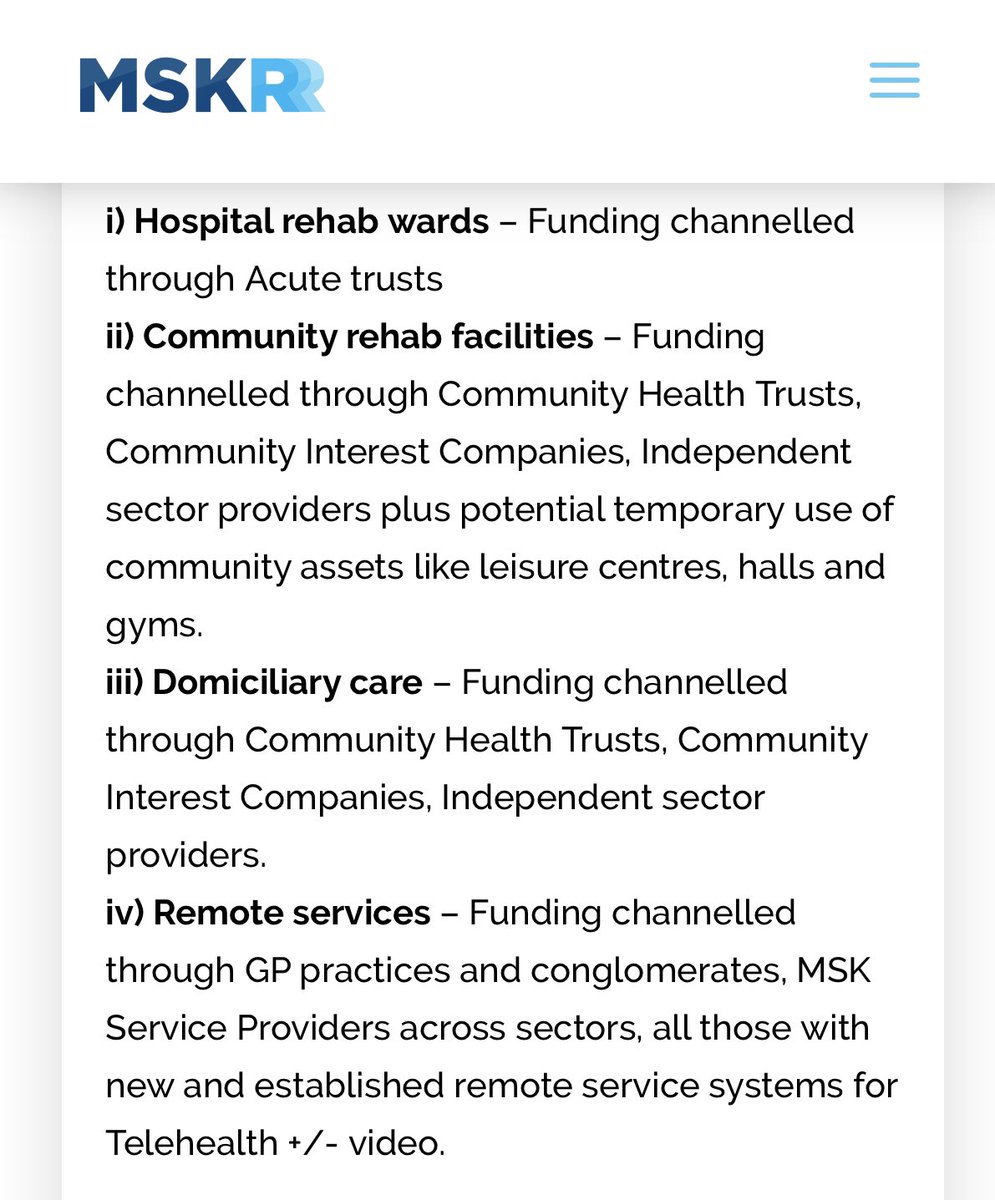
The operating model should include four overlapping care provisions beyond the acute setting:
i) Hospital rehab wards
ii) Community rehab facilities
iii) Domiciliary care
iv) Remote services
The more integrated the model, the smoother the step-up and step down transitions. 4/
i) Hospital rehab wards
ii) Community rehab facilities
iii) Domiciliary care
iv) Remote services
The more integrated the model, the smoother the step-up and step down transitions. 4/
Funding & employment model could follow the Nightingale hospitals (centrally funded infrastructure, NHS Profs employing)
But I think a better model would be to bolster existing service provisions through local CCG channels to manage infrastructure & employ the new workforce. 5/
But I think a better model would be to bolster existing service provisions through local CCG channels to manage infrastructure & employ the new workforce. 5/
Workforce - Big MDT with more role overlap than separation.
Use MSK, community, neuro rehab staff whose work has been changed most. Recruit other MSK Therapists from the private sector if they are Ev-informed and rehab-focussed (Sports Rehab & therapy, Osteos, Pods, Chiros) 6/
Use MSK, community, neuro rehab staff whose work has been changed most. Recruit other MSK Therapists from the private sector if they are Ev-informed and rehab-focussed (Sports Rehab & therapy, Osteos, Pods, Chiros) 6/
Grass-Roots MSK Think-Tank @MSKReform launched our Rehab Recruits campaign three weeks ago and have signed up over 2,000 interested individuals with no external publicity.
Read more and sign up at: MSKReform.org.uk/RehabRecruits 7/
Read more and sign up at: MSKReform.org.uk/RehabRecruits 7/
Competency – Fundamental functional rehab principles should be at the heart of all care with an agreement to focus on the 80+% agreement between the professions and where the evidence base is strongest.
Upskill based on declared training needs and on Ax of previous role. 8/
Upskill based on declared training needs and on Ax of previous role. 8/
I have loved seeing folk from various clinicians like @ajciliaOT & @RachelBotell sharing ideas under #COVIDrehab. Great hunger for rehab principles to underpin future care. 👌
If links could be made to the recent #RightToRehab lobbying efforts perhaps momentum could build?🤞9/
If links could be made to the recent #RightToRehab lobbying efforts perhaps momentum could build?🤞9/
INTEGRATE IT!
Why not link post-covid rehab with the care of those whose needs have not been met due to system disruption?
This also takes the opportunity for services to return to their prior function, if not improved, far quicker than a COVID specific pathway. 10/
Why not link post-covid rehab with the care of those whose needs have not been met due to system disruption?
This also takes the opportunity for services to return to their prior function, if not improved, far quicker than a COVID specific pathway. 10/
Is all this necessary? 🤷♂️
Is it feasible? 🤷♂️
Is there the political will? 🤷♂️
Can we shelf the inter-prof tribalism? 🤷♂️
Would LOVE to hear your thoughts!
Thanks to @rachaelmoses, @jo_khir, @alicecamurray, @_JoeMiddleton & @ScottBuxton_1 for informing my ponderings on this 👊/END
Is it feasible? 🤷♂️
Is there the political will? 🤷♂️
Can we shelf the inter-prof tribalism? 🤷♂️
Would LOVE to hear your thoughts!
Thanks to @rachaelmoses, @jo_khir, @alicecamurray, @_JoeMiddleton & @ScottBuxton_1 for informing my ponderings on this 👊/END