
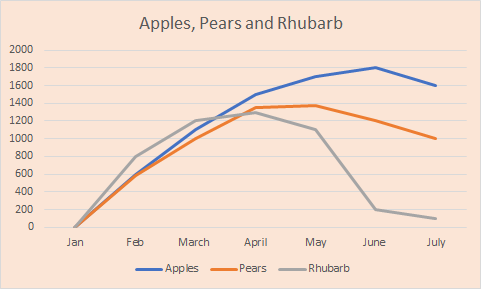
I've been inspired to initiate a debate about the comparisons in outcomes between different countries in their efforts to deal with the corona virus pandemic, by this graph posted by James Barr./1 
First my credentials. I founded the first cancer clinical trial's centre in the UK 1981 and directed it in various iterations for 30 years. I have no political affiliation and am driven by science. I'm an experimental clinical scientist not an epidemiologist. 2/
Epidemiology is observational science and is good at detecting associations between environmental and behavioural factors and links with disease. Association does not prove causation but is valuable in generating hypotheses to be tested in clinical trials (RCTs).3/
One exception to that is tobacco and lung cancer but there we had a relative risk x 40 whereas most "risk factors" are in the region 1.5-2.5. The association of this new corona virus with the COVID-19 pandemic is beyond question. 4/
Primary outcome measures foe RCTs are all cause mortality and quality of life. All other outcome measures are surrogate.
I will later explain why cause specific mortality in the time of this plague is unreliable. 5/
I will later explain why cause specific mortality in the time of this plague is unreliable. 5/
Comparing outcomes in this pandemic between different countries is, as suggested by James Barr, is like comparing Apples, pears and rhubarb. There are so many confounding variables I don't know where to start but I've put together some of them for starters. 6/
1. Population density
2. National demographics including incidence of co-morbidity.
3. A single or multiple epicentres for the start of the epidemic
4. Recording of incidence of infection
5. Recording cause specific or all cause deaths
6. Deaths from collateral fall out. 7/
2. National demographics including incidence of co-morbidity.
3. A single or multiple epicentres for the start of the epidemic
4. Recording of incidence of infection
5. Recording cause specific or all cause deaths
6. Deaths from collateral fall out. 7/
1. Pop density NZ 18/square KM v UK 430/ square Km
2. Some minority groups in rich countries have much co-morbidity
3. South Korea had one epicentre so they could track contacts easily
4. The more tests the higher the incidence. 8/
2. Some minority groups in rich countries have much co-morbidity
3. South Korea had one epicentre so they could track contacts easily
4. The more tests the higher the incidence. 8/
5. Quality of death registries vary between countries and many deaths from the virus will be away from hospital.
6. Collateral deaths, for example cancer, might be a consequence of redistribution of resources and deaths from say suicide might increase in lock down. 9/
6. Collateral deaths, for example cancer, might be a consequence of redistribution of resources and deaths from say suicide might increase in lock down. 9/
So far we've only discussed deaths at the time of the plague but we need to take the long view. The financial consequences of longer lock downs v shorter lock down might lead to more unemployment and poverty and that is the greatest determinant of longevity.

