
Algorithmic Necropolitics: Race, Disability, and Triage Decisionmaking
The algorithm that will decide who gets access to life saving care in the Commonwealth of Massachusetts was laid out on Apri 7th in this document: "Crisis Standards of Care Planning Guidance for the COVID-19 Pandemic" d279m997dpfwgl.cloudfront.net/wp/2020/04/CSC…
At first, it sounds good, because the authors claim that "the Commonwealth’s approach to crisis standards of care is that such tragically difficult decisions must be based on criteria that ensure that every patient has equitable access to any care from which they might benefit."
But then it goes on: "These criteria must be as clear,
transparent, and objective as possible, and must be based on biological factors related only to the likelihood and magnitude of benefit from the medical resources."
transparent, and objective as possible, and must be based on biological factors related only to the likelihood and magnitude of benefit from the medical resources."
And continues: "Factors that have no
bearing on the likelihood or magnitude of benefit, including but not limited to race, disability,
gender, sexual orientation, gender identity, ethnicity, ability to pay, socioeconomic status,
perceived social worth, perceived quality of life..
bearing on the likelihood or magnitude of benefit, including but not limited to race, disability,
gender, sexual orientation, gender identity, ethnicity, ability to pay, socioeconomic status,
perceived social worth, perceived quality of life..
... immigration status, incarceration status, homelessness or past or future use of resources, are irrelevant and not to be considered by providers making allocation decisions."
Why is this a problem?
Why is this a problem?
I'll get into some of the details in a moment, but here is the short version: If you think that health outcomes are 'based only on biological factors' then you are ignoring the key paradigm shift to social determinants of health (google it, or see cdc.gov/socialdetermin…)
Put another way, the authors of Crisis Standards of Care in MA are saying "Well, we don't see race / class / disability!"
This is despite the widely reported and increasingly understood reality that Black and Brown folks in MA, as elsewhere, are at much higher risk from Covid19. See dotnews.com/2020/city-repo… and bostonglobe.com/2020/04/09/nat…
But what does this have to do with Algorithms, you ask?
Well, an algorithm is a set of rules to be followed in calculations or other problem-solving operations.
Here is how the proposed Crisis Standards of Care algorithm works:
Well, an algorithm is a set of rules to be followed in calculations or other problem-solving operations.
Here is how the proposed Crisis Standards of Care algorithm works:
From p14, triage steps:
1. Calculat[e] each patient’s priority score based on the multi-principle allocation framework;
2. Assign each patient to a [color coded] priority group;
3. Determin[e] on a frequent basis how many priority groups will receive access to critical care.![This triage process involves several steps, detailed below: <br />
<br />
<span class=]() 1. Calculating each patient’s priority score based on the multi-principle allocation framework;
1. Calculating each patient’s priority score based on the multi-principle allocation framework;
2. Assigning each patient to a priority group (to which hospitals may assign color codes); and
3. Determining on a frequent basis how many priority groups will receive access to critical care interventions." src="/images/1px.png" data-src="https://pbs.twimg.com/media/EVgrgyeXQAMUj-Z.png">
1. Calculat[e] each patient’s priority score based on the multi-principle allocation framework;
2. Assign each patient to a [color coded] priority group;
3. Determin[e] on a frequent basis how many priority groups will receive access to critical care.
 1. Calculating each patient’s priority score based on the multi-principle allocation framework;
1. Calculating each patient’s priority score based on the multi-principle allocation framework;2. Assigning each patient to a priority group (to which hospitals may assign color codes); and
3. Determining on a frequent basis how many priority groups will receive access to critical care interventions." src="/images/1px.png" data-src="https://pbs.twimg.com/media/EVgrgyeXQAMUj-Z.png">
As they say, "This allocation framework is based on two considerations: 1) saving the most lives; and 2) saving the
most life-years."
most life-years."
"Patients who are more likely to survive with intensive care are prioritized over patients who are less likely to survive with intensive care. Patients who do not have serious comorbid illness are given priority over those who have illnesses that limit their life expectancy."
Points are assigned for SOFA score category (1-4 points) and the presence of comorbid conditions (2 points for major life-limiting comorbidities, 4 points for severely life-limiting comorbidities).
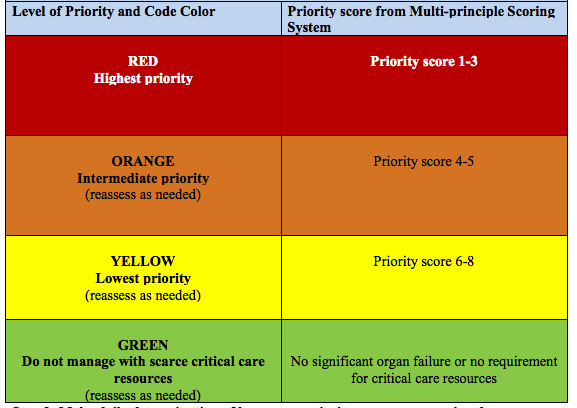
"These points are then added together to produce a total priority score, which ranges from 1 to 8. Lower scores indicate higher likelihood to benefit from critical care; priority will be given to those with lower scores." 

Once you've been given a total priority score, which will be higher for each condition you might have that reduces your change for long-term survival, you get a color coded priority: "Step 2- Use Priority Score from Multi-principle Scoring System to Assign Priority Category"
So that's the part where we have a proposed algorithm ("a set of rules to be followed in calculations or other problem-solving operations") that will be used for life-critical triage decisionmaking. But what's necropolitics, and what does this have to do with race and disability?
Necropolitics is a term, developed by Cameroonian philosopher and political theorist Achille Mbembe, to describe the various kinds of social and political power that dictate how and whether people live or die, and under what conditions their bodies will exist.
The Proposed Crisis Standards of Care is a necropolitical document because it lays out the algorithm that will allocate scarce resources to some bodies and deny them to others. It's about race & disability b/c its point system is implicitly racist and explicitly ablist.
Implicitly racist, because it pretends to be 'colorblind' despite everything we know about how social determinants of health (especially race) structure risk for conditions that are considered comorbidities (diabetes mellitus, chronic lung disease, and cardiac disease)
Explicitly ableist, because many disabilities will give patients a higher SOFA point score and/or a higher point score on prognosis for long-term survival (and thereby reduce likelihood that those patients are assigned to a higher priority group).
In response to this harmful algorithm masked as equitable triage, over 100 doctors, nurses, and other medical professionals in MA have launched an Open Letter to the Crisis Standards of Care Advisory Committee: docs.google.com/document/d/13k…
They note that "This committee had little to no representation from the communities most impacted by COVID-19 and had no community oversight. Only two of the sixteen authors were people of color."
As they point out, "health conditions that directly or indirectly factor into the SOFA scoring system are disproportionately high among Boston’s communities of color [...] diabetes rates are highest in Mattapan (17.3%), Roxbury (14.1%), and Dorchester (12.8%).
"Dorchester, Mattapan, Roxbury, and Hyde Park have the highest percentage of both diabetes-related and heart disease-related hospitalizations among Boston neighborhoods."
"Due to a well-documented presence of housing and environmental triggers (e.g. mold hazards/violations, poor indoor air quality), asthma-related illnesses are disproportionately high in Dorchester, Mattapan, and Roxbury, placing residents in those neighborhoods at increased risk"
Later in the letter, they point out that "Black, Latinx, and Asian populations are at heightened risk of contracting COVID-19 and exposing their families given overrepresentation as essential, frontline workers."
Also, "Another group of people at higher risk of acquiring COVID-19 are correctionally-involved/incarcerated individuals who must live in crowded conditions and bear a higher burden of comorbid conditions as compared to the general population." ...
"Since mass incarceration is driven by racial and economic injustice, Crisis Standards of Care need to take into consideration that those individuals who are put at risk for COVID-19 because of their identities and socioeconomic status" ...
... "will also be the ones who will be further penalized by the scoring system due to comorbid conditions acquired during incarceration."
They then cite nobodyisdisposable.org/open-letter/ re: “denying or withdrawing care based on protected characteristics violates many laws including the Americans with Disabilities Act, Section 504, the Affordable Care Act, state and local civil rights laws, and/or the U.S. Constitution.”
The open letter ends with a set of demands, first:
1) Just and ethical crisis standards that take into account political and social determinants of health to assure truly equitable allocation of resources;
Please read the rest for yourself: docs.google.com/document/d/13k…
/end
1) Just and ethical crisis standards that take into account political and social determinants of health to assure truly equitable allocation of resources;
Please read the rest for yourself: docs.google.com/document/d/13k…
/end
[Fixing broken thread]
[Fixing the thread again]:
PS H/T to R. Joshua Scannell (@joshscann), who wrote about algorithmic necropolitics in Ch. 5 of Captivating Technology, ed. by @ruha9, here: static1.squarespace.com/static/5b5b473…

