
Ok, I have to say something, especially as I keep getting pulled into in these posts. COVID-19 causes ARDS. I keep hearing the refrain that it is not ARDS because “the compliance is normal.”
Yet, I have not seen a single person proclaiming this share their institution’s average compliance (much less the n from which it was calculated.) They go back to Dr. Gattinoni’s letter to the editor, reviewing their experience with 16 patients.
In that letter, the average compliance was 50 mL/cmH2O. You know who else has a compliance pretty close to 50? Patients with ARDS. Don’t believe me? Look at Table 1 from Dr. Gattinoni’s NEJM publication in 2006.
44 for the entire group, 49 for the lower percent recruitable group and 40 for the higher-recruitability group. 
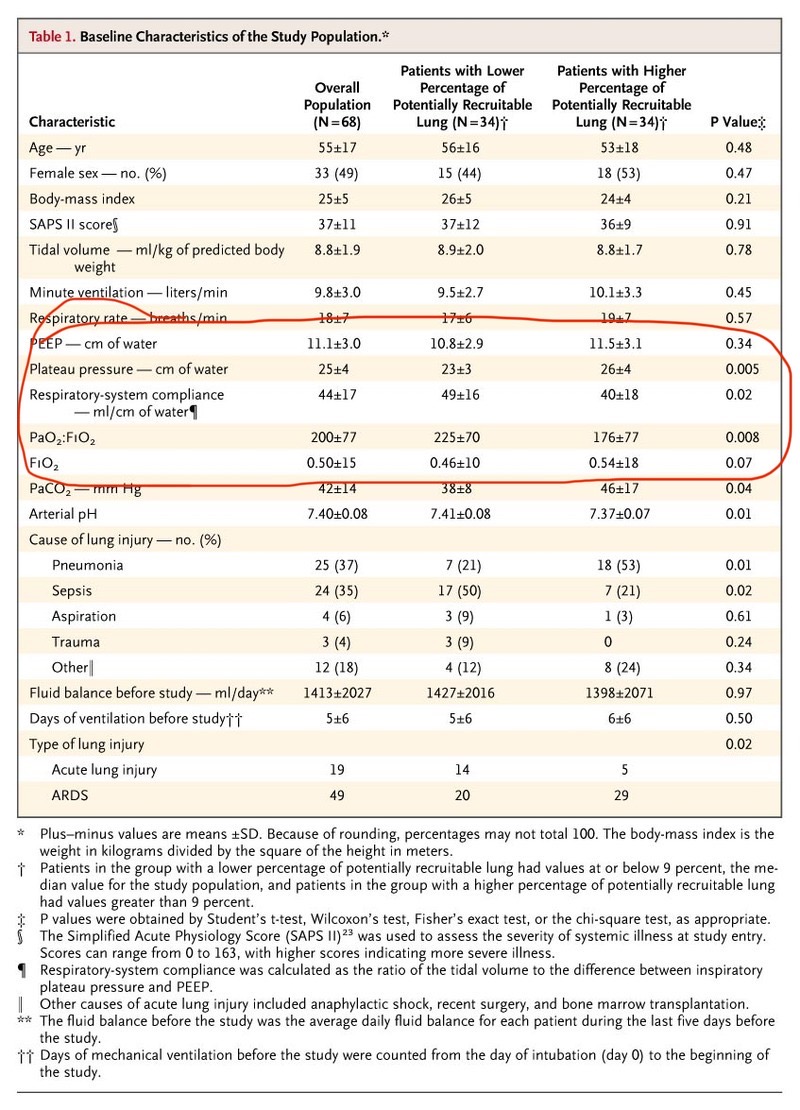
Did you catch that too? That patients with ARDS have variations in their recruitability is well-known. That’s what Dr. Gattinoni shows in that paper. Here’s the reference. nejm.org/doi/full/10.10…
Also, the report of 23 patients from Seattle found a compliance of 29. Not normal. nejm.org/doi/full/10.10… Intensivists have long known that patients with ARDS have markedly varied presentations. The variations just seem stark and the outliers more obvious because of the volume.
If you want to see a fascinating manuscript on the histopathology of COVID-19, look at this. Two patients were accidentally taken to the OR for lung resections with early COVID-19, before either had classic symptoms. jto.org/article/S1556-…
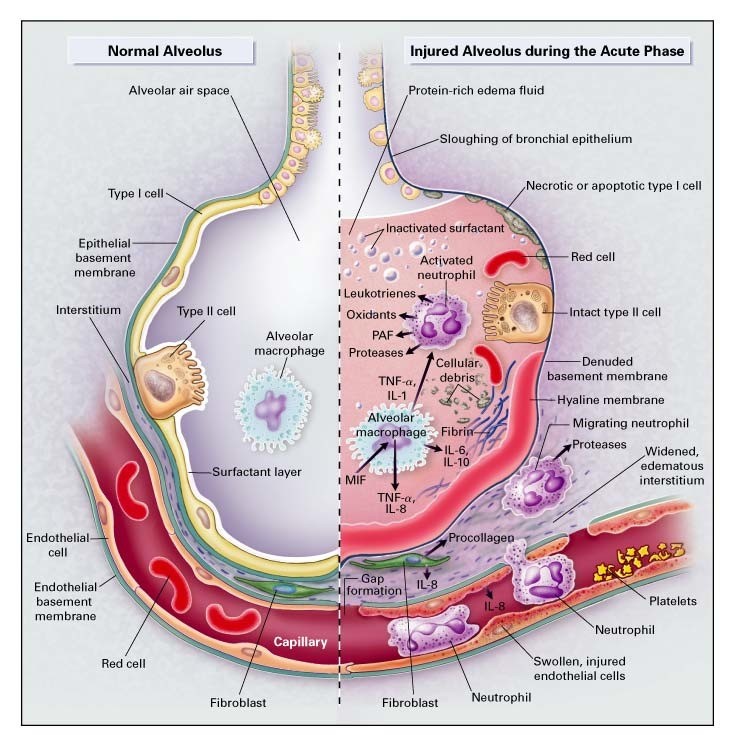
They showed edema and prominent proteinaceous exudates, vascular congestion, and inflammatory clusters with fibrinoid material and multinucleated giant cells. Here is the classic picture of ARDS from the NEJM. Anything sound familiar? nejm.org/doi/full/10.10…
Furthermore, none of this supports the contention that it is fine to allow patients with low O2 sats to sit with profound hypoxemia. Where is this coming from? What data supports this practice?
The most recent trial of conservative vs liberal O2 targets was stopped early because of no benefit to conservative strategy – and concern for harm. nejm.org/doi/pdf/10.105… We know that self-induced lung injury occurs – and is what Dr. Gattinoni warns against in his editorial.
And, those saying that the ventilator itself is causing harm seem to be confusing correlation with causation. The vast majority of patients with COVID-19 do not need to be intubated. Those who do are the sickest of the sick.
Getting patients off the ventilator is what we intensivists do. If patients don’t need to be ventilated, we assess them, turn down the support, and extubate. Patients who stay intubated do so for a reason.
This is a bad condition, often with poor outcomes if it gets to the point of requiring intubation. It does not necessarily follow, however, that withholding intubation improves outcomes.
I'm not saying that we have no room to improve, no room to learn. Of course we do. We always do. But this is not the time to abandon 25 years of well-done research in favor of anecdotes and opinions - many of which are promulgated without even offering biological plausibility.

