
Can tracing alone control COVID?
Our model: it's possible if we >double efficacy by changing how we trace & use digital apps.
Thanks to @willbradbio, @EthanAlley, @jhhhuggins, & epidemiologist @alun_l !
doi.org/10.1101/2020.0…
1/n
Our model: it's possible if we >double efficacy by changing how we trace & use digital apps.
Thanks to @willbradbio, @EthanAlley, @jhhhuggins, & epidemiologist @alun_l !
doi.org/10.1101/2020.0…
1/n

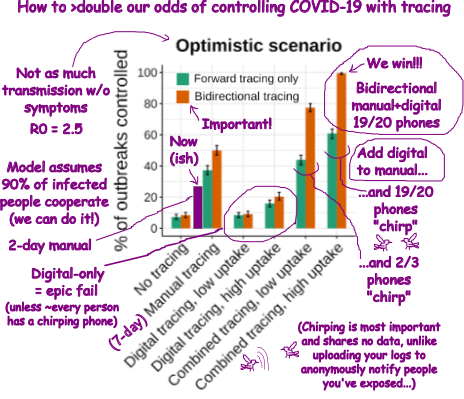
Tl;dr: We need bidirectional tracing to find infectors and undiagnosed carriers, and almost everyone’s smartphones should “chirp”. Combined = we win… in the optimistic scenario. Else add masks or distancing.
2/n
2/n
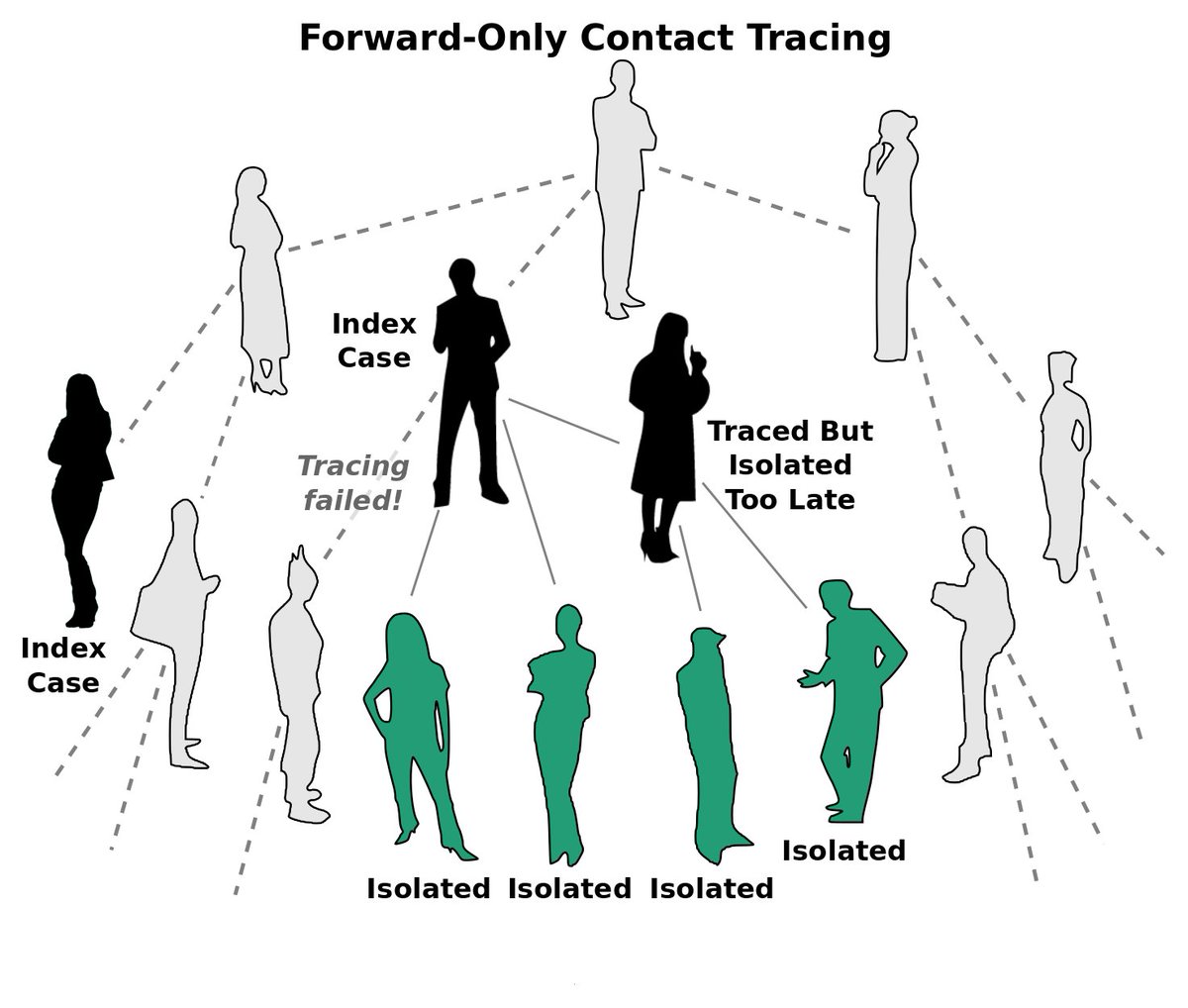
Right now, we “forward-trace” to find and isolate people who were exposed so they don’t infect anyone else.
Problem: many cases are undiagnosed, especially if asymptomatic, so we miss branches of the viral family tree.
3/n
Problem: many cases are undiagnosed, especially if asymptomatic, so we miss branches of the viral family tree.
3/n
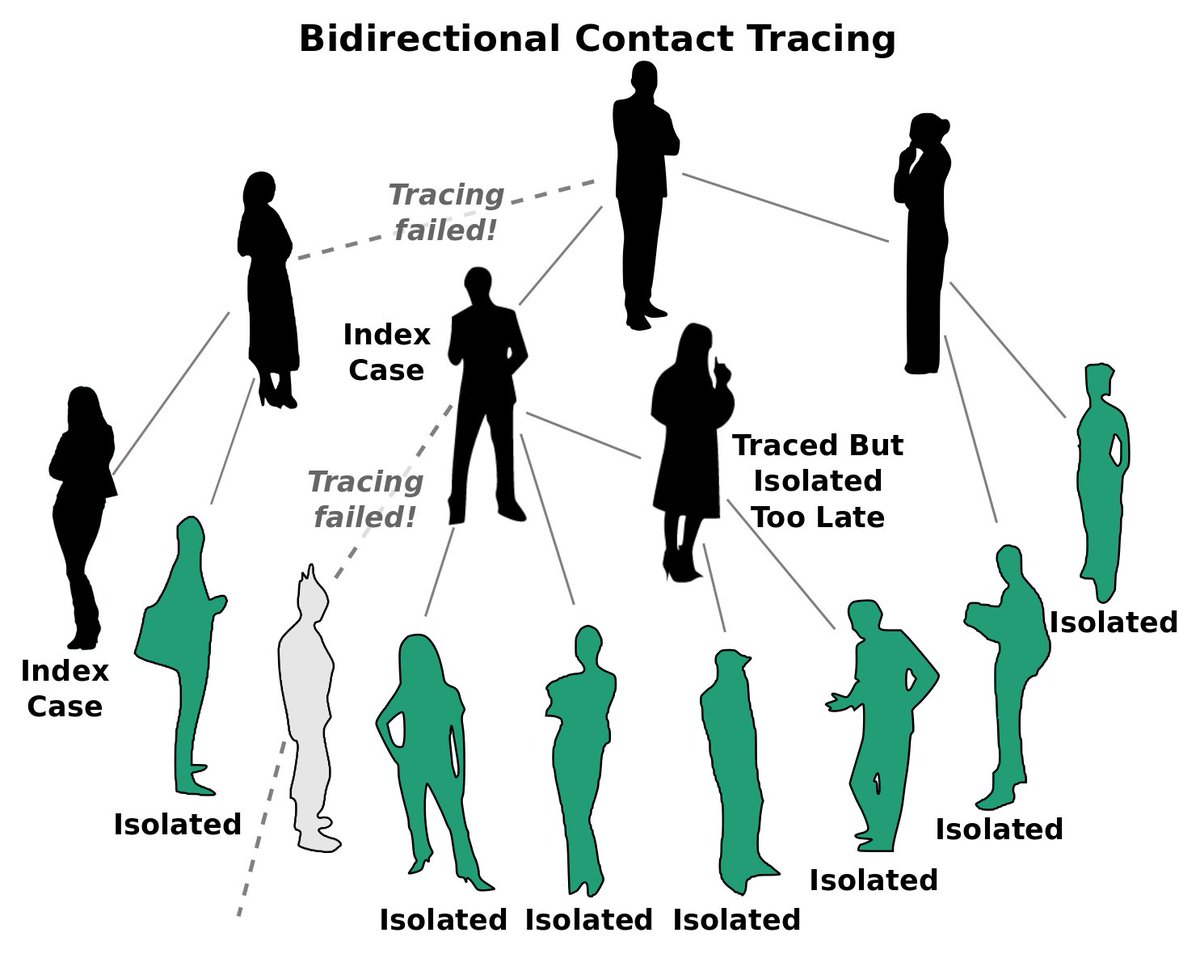
We reasoned that iterative “bidirectional” tracing could find and isolate these unknown branches. Since asymptomatic COVID may be common (could be age-dependent), it might make a big difference.
4/n
4/n
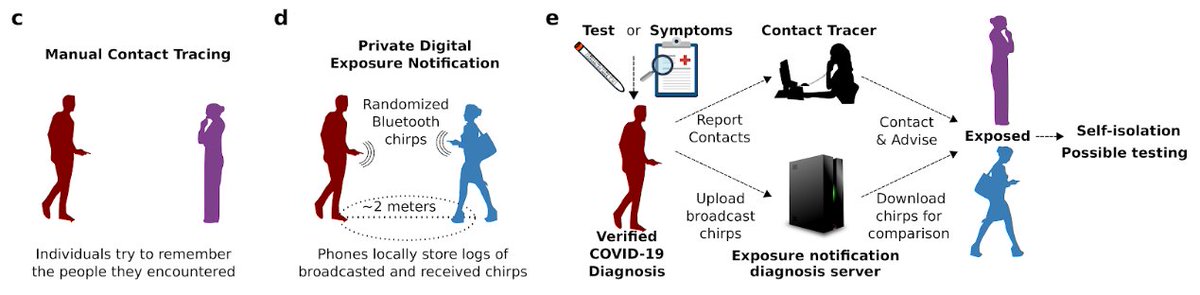
Tracers are overburdened, so adding bidirectional would be a lot to ask. But digital methods that use randomized Bluetooth “chirps” could automate a lot of the work, letting people focus on cases without smartphones.
5/n
5/n
We (meaning @willbradbio, who is a master of R) adapted a stochastic branching process model of contact tracing to see how well bidirectional tracing worked, and how manual and digital squared up.
Original: thelancet.com/journals/langl…
6/n
Original: thelancet.com/journals/langl…
6/n
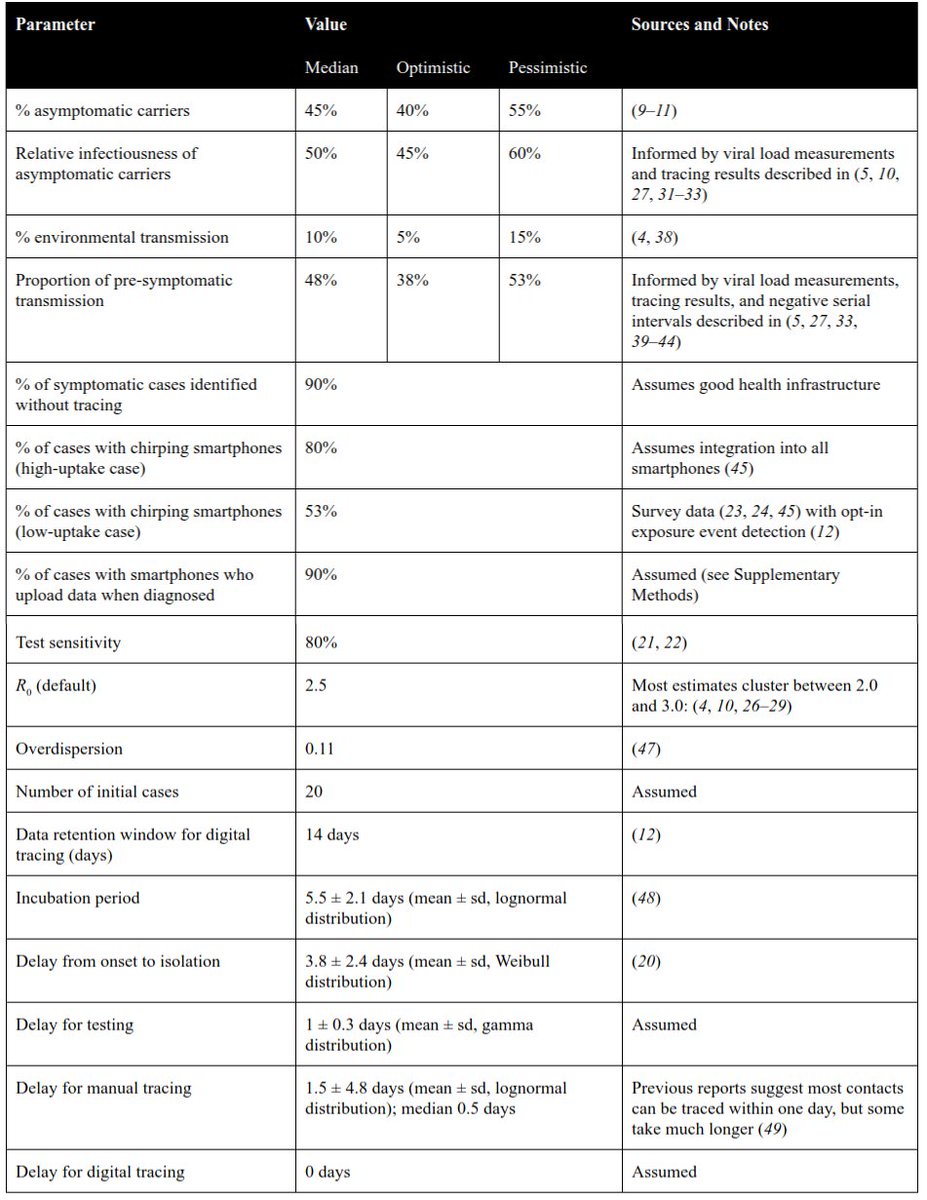
Data on epidemiological parameters varies a LOT. So we compiled studies and independently estimated each parameter, which we combined to come up with three scenarios of how much transmission occurs without symptoms. Median values:
7/n
7/n
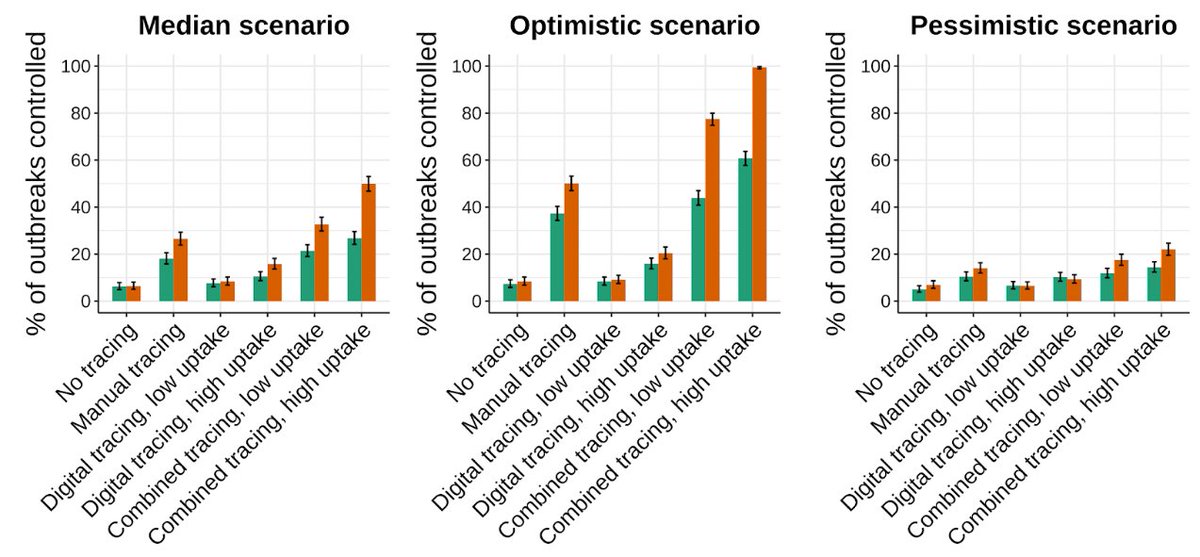
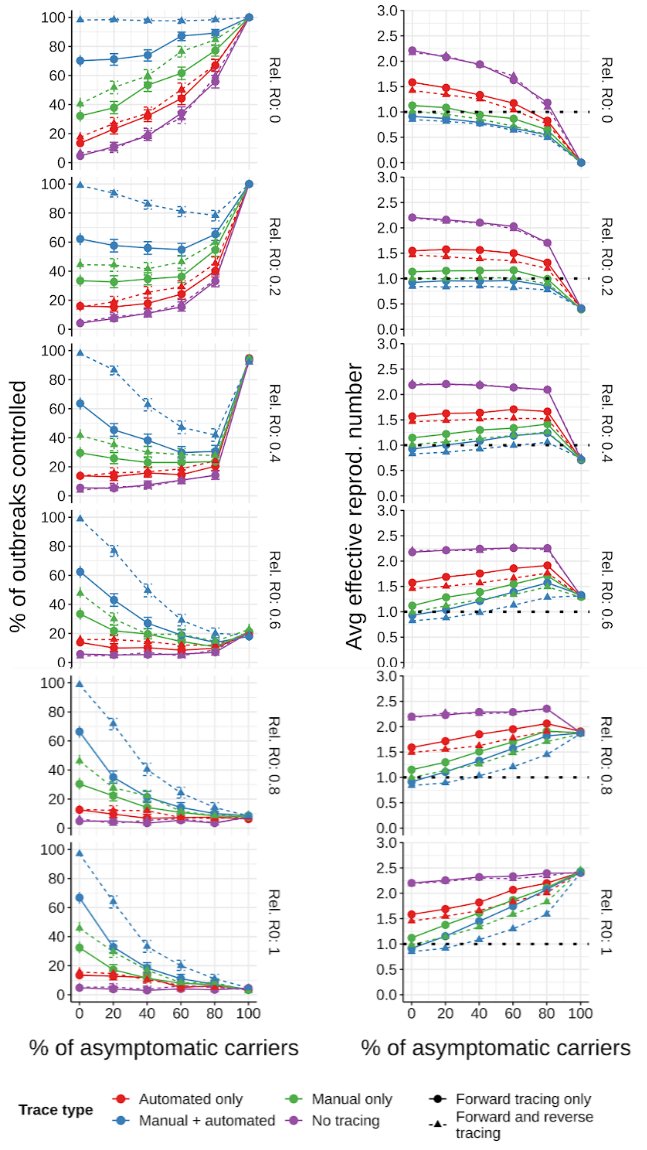
Median scenario results: manual forward-tracing alone, even improved (7 days w/ 98% success save env. transmission), doesn’t control COVID (also doesn’t in reality: check). Making it bidirectional helps a lot if tracing success is high.
8/n
8/n

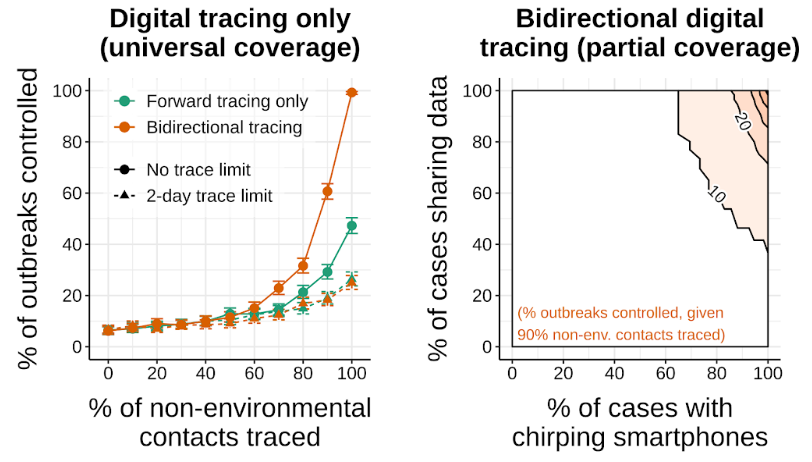
In contrast, digital-only looks AMAZING… until you look at what happens when less than ~100% of people have chirping smartphones or share their chirp logs when infected. Just ~2/3 say they’ll install an app. For now, digital-only = fail.
9/n
9/n
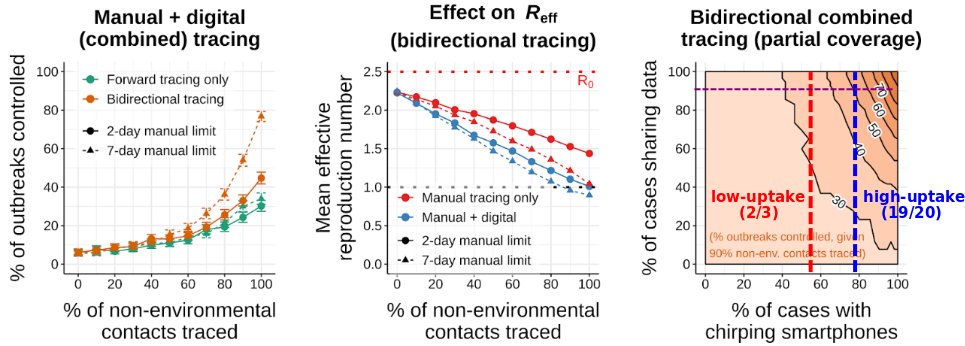
Combine digital and manual so the latter focuses on people w/o smartphones, and it looks far better, esp. if most existing phones chirp. >2x odds of control and lower R_eff. But low uptake (~2/3 smartphone users opt-in) is much worse.
10/n
10/n
But that’s just the median scenario. Optimistic looks quite a bit better & pessimistic a lot worse. R0 also matters. Note: our optimistic scenario is a bit more negative than most models. More on that later.
11/n
11/n
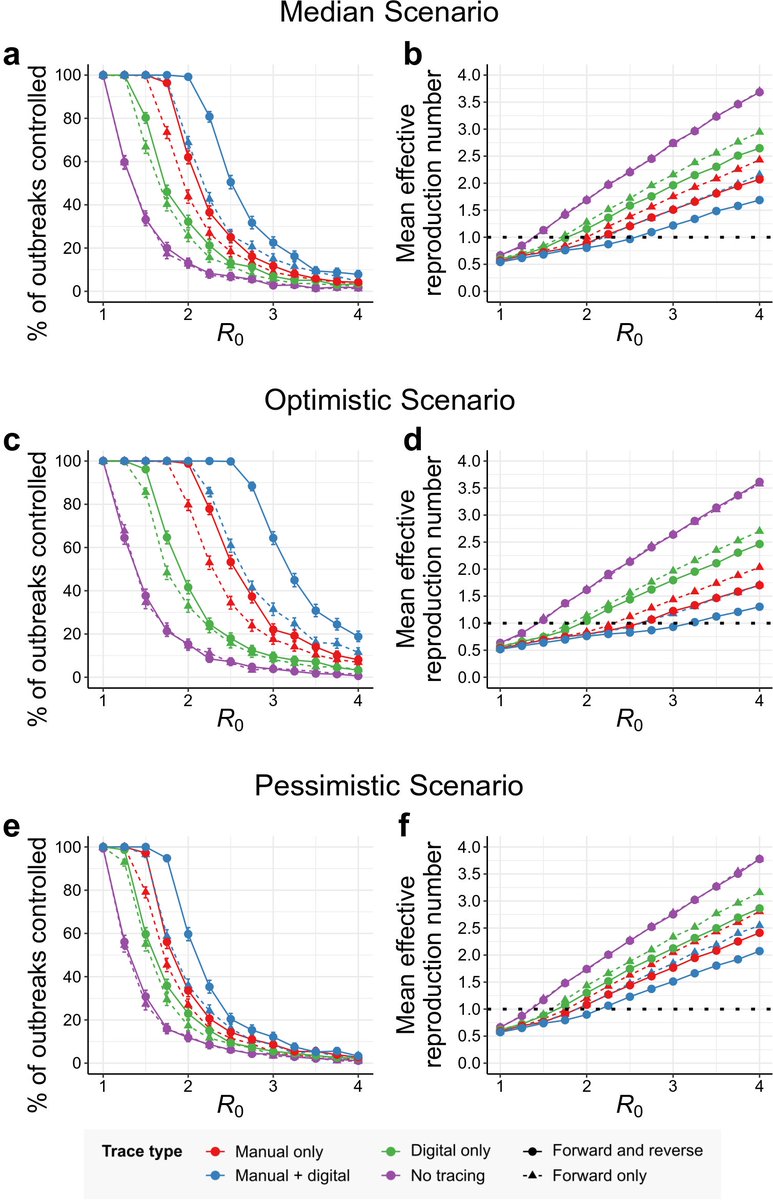
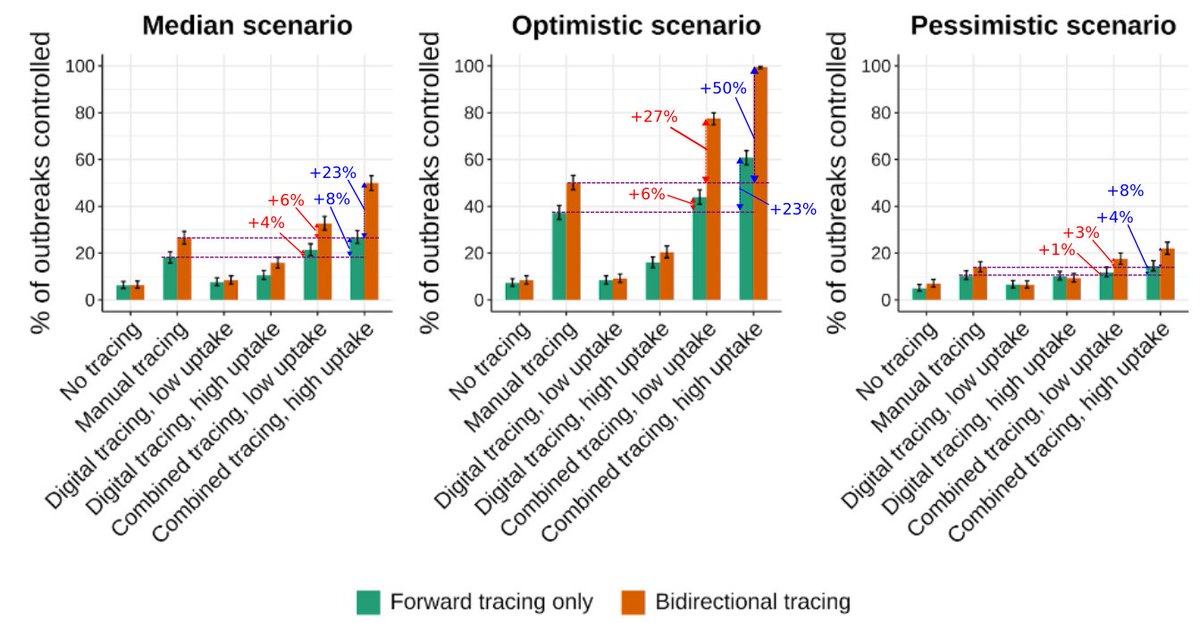
Okay, let’s go back to our summary, which was optimistic. What does it look like for median and pessimistic? Not so hot. But asking for high control probability is a lot. Fortunately we can convert to R.
12/n
12/n
Here are effective reproduction numbers across scenarios, same R0=2.5. Manual tracing out 7 days gets you far, especially bidirectional. In optimistic, almost below 1… e.g. ~50% odds of control. Bidirectional hybrid is always best.
13/n
13/n
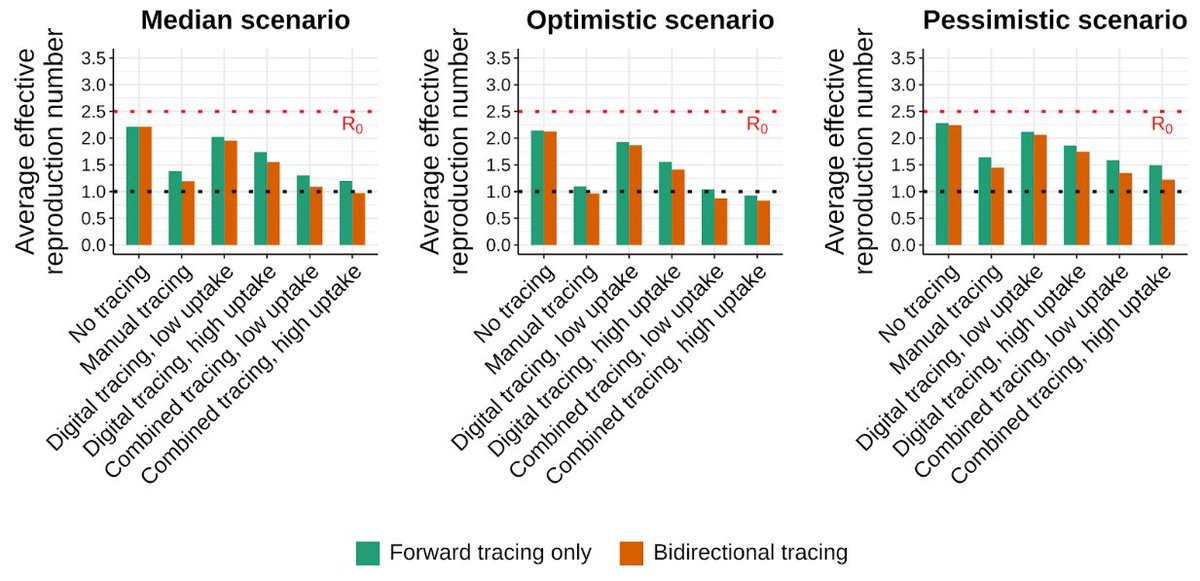
But uptake on digital is key. If randomized Bluetooth chirping is opt-in, and 2/3 to 3/4 of people do (per surveys), you get low-uptake. Adding low-uptake is little better than 7-day manual! We need almost everyone w/ a smartphone.
14/n
14/n
Overall, we think everyone should 1) use bidirectional tracing, 2) make nearly all smartphones chirp, and 3) enable voluntary decentralized sharing of anonymous chirp logs once infected to notify potential infectors/infectees.
15/n
15/n
So why is control so difficult with tracing in our scenarios vs others? Reports of high transmission without symptoms. For example, 40%+ of transmission likely occurs before symptoms onset, which matters.
16/n
16/n
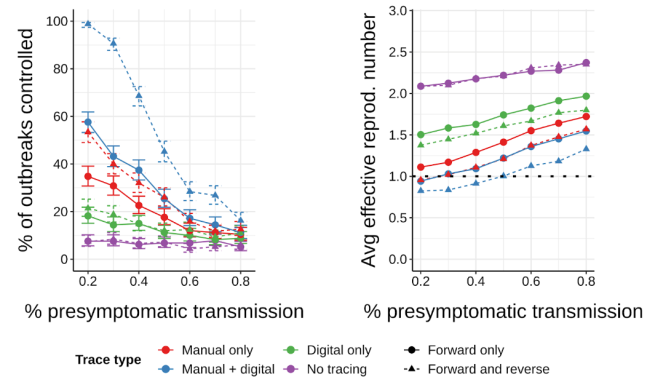
Similarly, there are likely 40%+ asymptomatics who are perhaps 50% contagious relative to symptomatics. We could be wrong in our estimates (and probably are), but we’d rather not be overly optimistic.
17/n
17/n
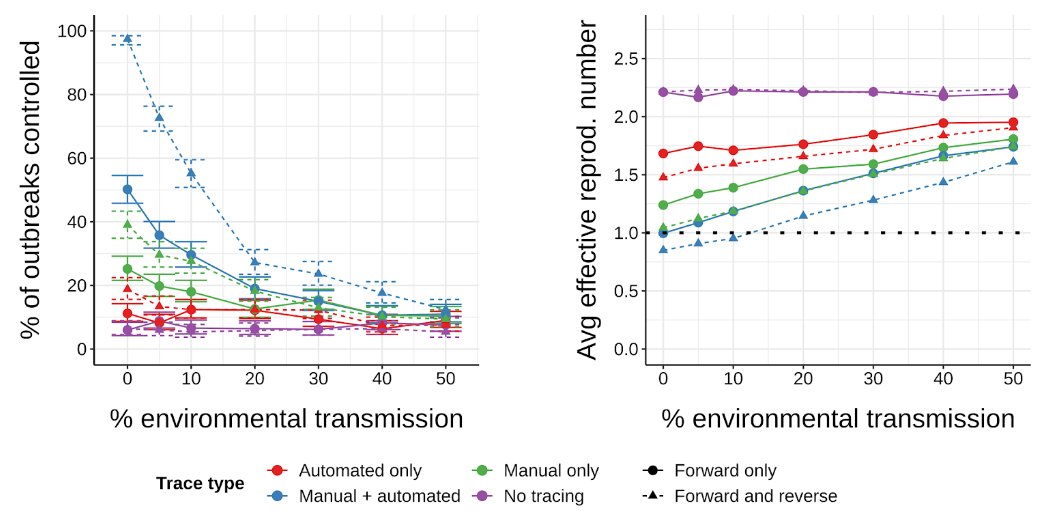
Another big one is environmental/surface transmission. We use 8-13%. If higher, contact tracing struggles. Other than the Wenzhou cluster we have little data, suggesting it's low overall, but how low matters a great deal.
18/n
18/n
Caveat: this is a preprint. If accurate, our findings should inform policy/development, but they're preliminary. If you've read this far, please read the manuscript and send feedback. With COVID, we can ill afford mistakes.
19/n
19/n
Lastly, thanks to my mother, my mother-in-law, and my wife, without whom this thread - and all my contributions to research - wouldn’t be possible.
All three are vulnerable or on the front lines. Let’s #BeatTheVirus.
20/20
All three are vulnerable or on the front lines. Let’s #BeatTheVirus.
20/20
(To anyone having trouble downloading the PDF from medRxiv, it's also available from our group's website)
sculptingevolution.org/publications
sculptingevolution.org/publications

