
Instead of my normal #GTScase, I wanted to look at the morphology of pediatric bone marrows for #hemepath. Following @CArnold_GI ‘s advice, I am going to make these unknowns. Let's take a look! 👀 
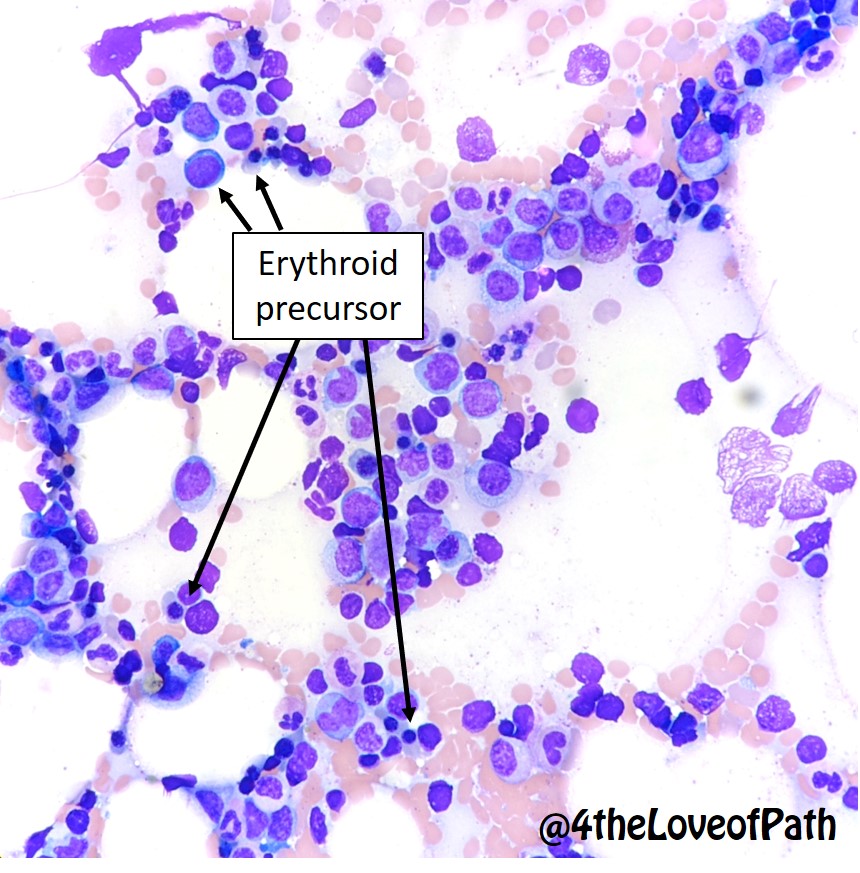
First, let’s review normal bone marrow morphology on core biopsies and aspirates.
1) Cellularity (% of cells in the space between trabeculae) 2) Trilineage hematopoiesis (megakaryocytes, granulocytes, erythrocytes) with myeloid:erythroid ratio (M:E)
3) Presence of blasts
1) Cellularity (% of cells in the space between trabeculae) 2) Trilineage hematopoiesis (megakaryocytes, granulocytes, erythrocytes) with myeloid:erythroid ratio (M:E)
3) Presence of blasts



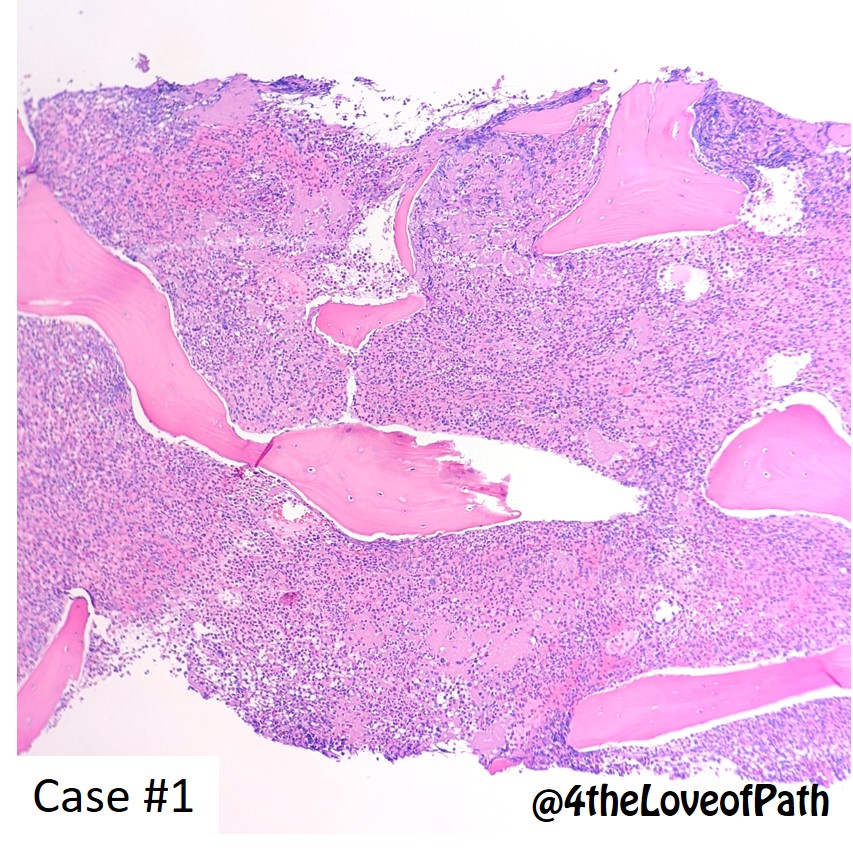
Case #1




Based on the morphology from the core biopsy, aspirate, and smear, what is your the diagnosis?
What markers would you expect to be positive on flow cytometry?
Case #1: Chronic myelogenous leukemia (CML). Key features: ⬆️⬆️WBC on peripheral smear +/- basophilia, myeloid precursors, aspirate with ⬆️myeloid cells, hypercellular marrow with ⬆️ M:E ratio, pseudo Gaucher cells may be seen with high cell turnover. **CD11b+ for basophils.**


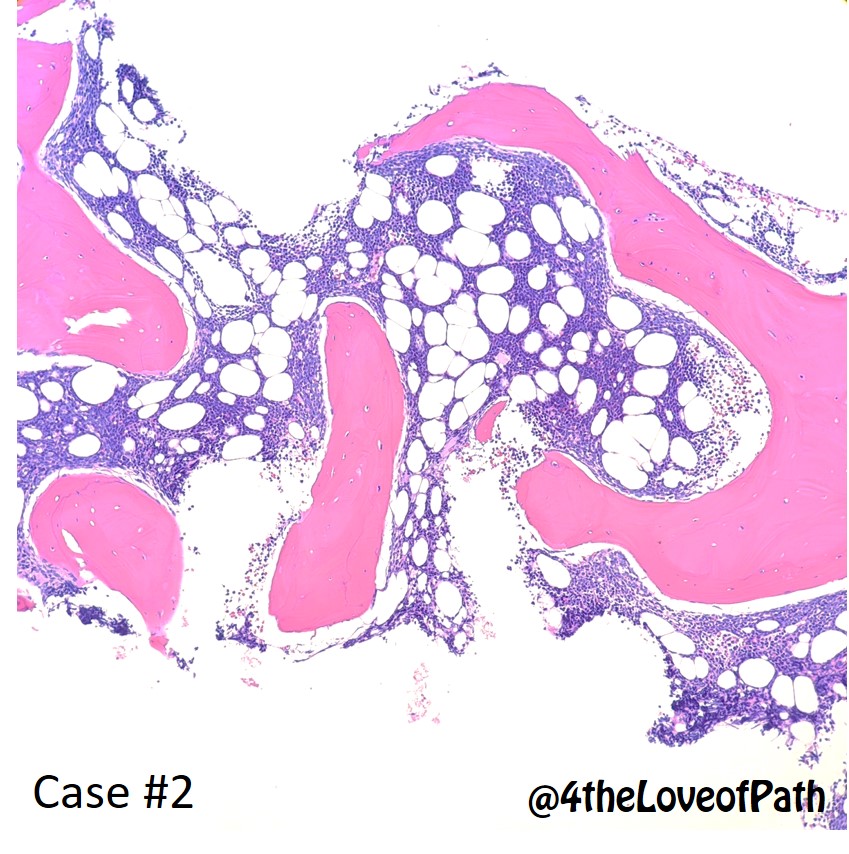
Case #2




Based on the morphology from the core biopsy, aspirate, and smear, what is your the diagnosis?
What markers would you expect to be positive on flow cytometry?
Case #2: Acute lymphoblastic leukemia (ALL). Key features: +/- blasts on peripheral smear, lymphoblasts in aspirate, cellular marrow with >20% blasts (very “purple” with high N:C ratio). **Size reference: Blasts are usually larger than RBCs or mature neutrophils**


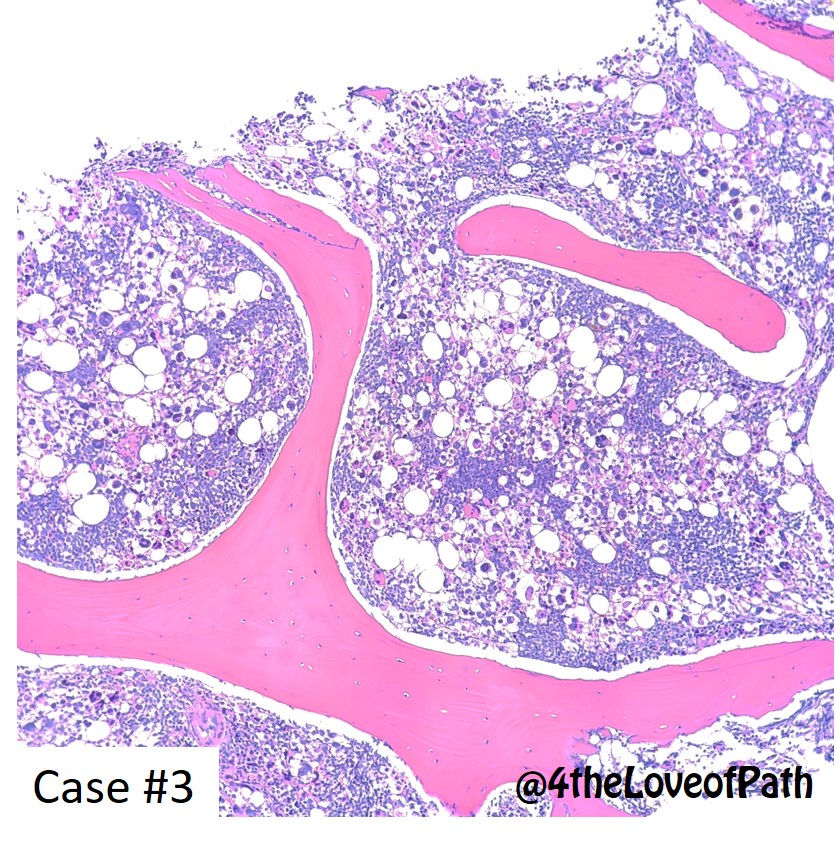
Case #3




Based on the morphology from the core biopsy, aspirate, and smear, what is your the diagnosis?
What markers would you expect to be positive on flow cytometry?
Case #3: Acute myelogenous leukemia (AML) w/ megakaryoblastic features. Key features: megakaryoblasts with blebbing on aspirate and smear, ⬆️ dysplastic megakaryocytes on biopsy. **IHC stains for CD31 can be very helpful if the blasts are not strongly CD61+ **




AML can have multiple differentiations, since the blasts are from the CSF-GEMM stem cell. Below is an example of monocytic AML. Note how the blasts look different from the ALL and megakaryoblastic AML cases.




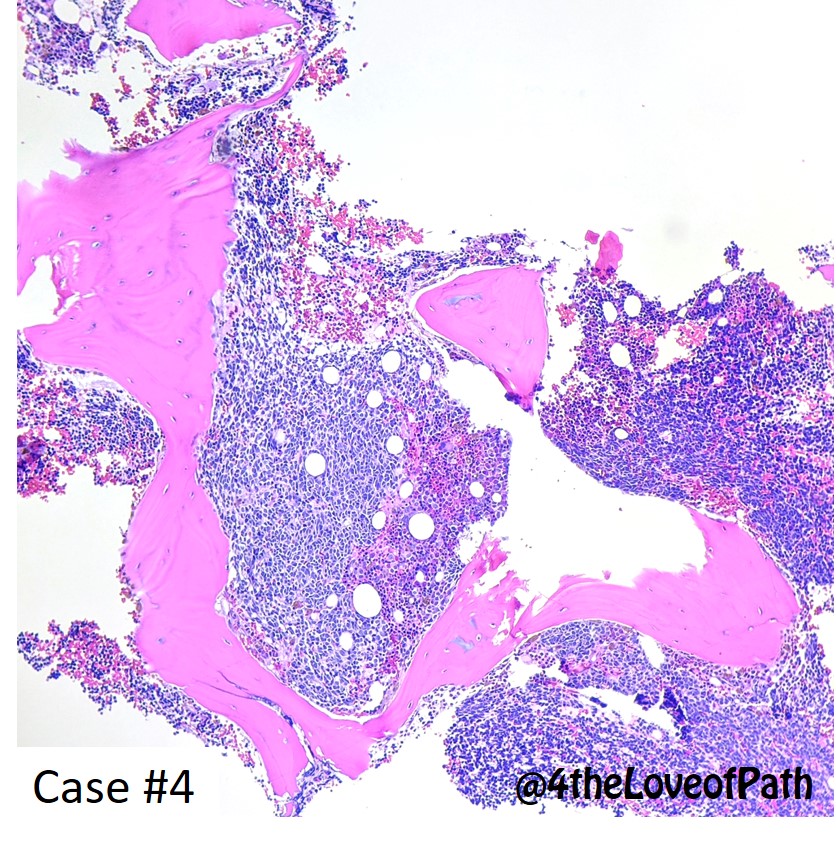
Case #4




Based on the morphology from the core biopsy, aspirate, and smear, what is your the diagnosis?
Instead of flow cytometry, what IHC stains would you consider ordering?
Case #4: Metastatic neuroblastoma. Key features: "Cohesive" clusters of cells on aspirate, similar small round blue cells on core. Previous h/o of malignancy is key. Stains are helpful for identifying the tumor, and assessing cellularity of tumor in marrow.




Thank you all for participating! If you have any questions, comments, or notice anything that is incorrect, let me know.
Not sure how well the tag function worked in the first tweet.
@KMirza @path_smalls @PathologySayah @Path_Matt @DrSamreenfatima
@KMirza @path_smalls @PathologySayah @Path_Matt @DrSamreenfatima

