1/ Do we make sure virus activity is low before reopening?
These policy experts say it's fundamental to #OpenSafely
That seems so obvious you may ask "who'd disagree? what's the alternative?"
I got the chance to debate @lanheechen on just that @cwclub
These policy experts say it's fundamental to #OpenSafely
That seems so obvious you may ask "who'd disagree? what's the alternative?"
I got the chance to debate @lanheechen on just that @cwclub
2/ First off, I'm grateful to @lanheechen @bobkocher @Bob_Wachter and especially @Avik for providing a detailed alternative strategy-we need to be able to debate and simply saying "America needs to get back to work" is not a strategy
The @FREOPP proposal
freopp.org/a-new-strategy…
The @FREOPP proposal
freopp.org/a-new-strategy…
3/ They start w 3 assertions (I half agree)
(1) significant possibility of a pessimistic scenario with respect to vaccines and treatments in the near term
(2) heavy skew of death from COVID-19 toward the elderly/ those with chronic disease
(3) new tools for contact tracing
(1) significant possibility of a pessimistic scenario with respect to vaccines and treatments in the near term
(2) heavy skew of death from COVID-19 toward the elderly/ those with chronic disease
(3) new tools for contact tracing
4/ And they deduce that we need to be more aggressive about reopening, especially with reopening K-12, lift stay-home orders for non-elderly, reduce risk at workplaces, etc and focus on nursing homes
kind of like Sweden (which BTW I'm also grateful for having as an alternative)
kind of like Sweden (which BTW I'm also grateful for having as an alternative)
5/ Here's my fundamental Q to @lanheechen about this approach that I don't think I ever got answered
Are you assuming that the outbreak never flares among the young, or that it's OK to get to 30-60% infection rates?
(you can watch the entire debate here )
Are you assuming that the outbreak never flares among the young, or that it's OK to get to 30-60% infection rates?
(you can watch the entire debate here )

6/ My view is that you can NEVER allow exponential growth on a high base of cases
So you only reopen (increase R) if you KNOW that
*the rate of active infection is low
*R is low
*you have something to replace lost R suppression
*you can detect a change quickly
*can deal w surge
So you only reopen (increase R) if you KNOW that
*the rate of active infection is low
*R is low
*you have something to replace lost R suppression
*you can detect a change quickly
*can deal w surge
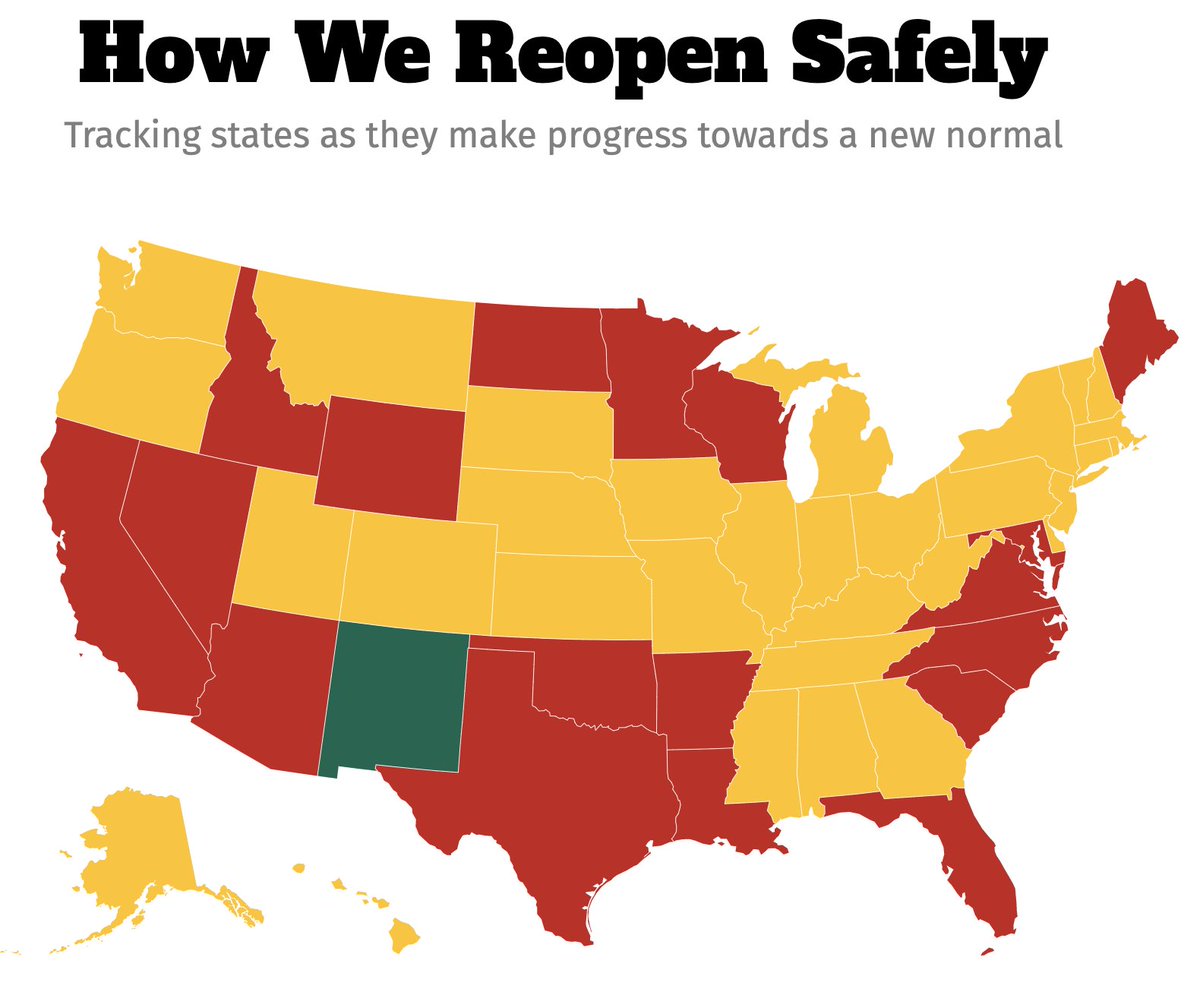
7/ That's basically what all the epi-driven reopening plans are trying to do, even if they aren't explicit about the framework
The best place to see this data (incl missing) at state level is, alas, not the @CDCgov right now, it's covidexitstrategy.com
The best place to see this data (incl missing) at state level is, alas, not the @CDCgov right now, it's covidexitstrategy.com
8/ But the @freopp plan has no such gating criteria and @Avik has been clear that it's a feature of his plan
@lanheechen "Sure, everyone wants more information. But have to open to keep people in work."
maybe @Bob_Wachter and @bobkocher signed on to it without realizing that?
@lanheechen "Sure, everyone wants more information. But have to open to keep people in work."
maybe @Bob_Wachter and @bobkocher signed on to it without realizing that?
9/ So what's the thinking?
It's not explicit, but it seems to be: "sure, let's do our best to do harm reduction and slow down the spread among younger/healthier folks, but their death rate is so low, it's not a big deal if it does spread"
"less than flu"
It's not explicit, but it seems to be: "sure, let's do our best to do harm reduction and slow down the spread among younger/healthier folks, but their death rate is so low, it's not a big deal if it does spread"
"less than flu"
10/ The problem with this argument is that at COVID is much worse than flu, even for non-elderly
If you let er rip in society at large, there will be a huge health/economic impact
And no, I don't think we can effectively segregate old people
If you let er rip in society at large, there will be a huge health/economic impact
And no, I don't think we can effectively segregate old people
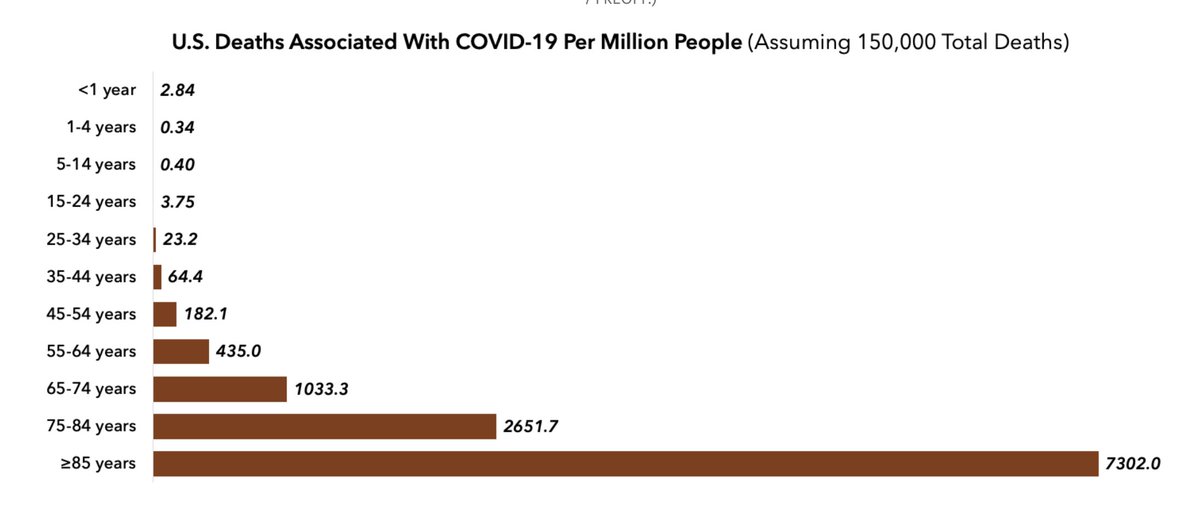
11/ This analysis starts with ASSUMING 150k deaths.
But if we allow exponential growth on a high base, if allow high proportion of general population to become infected, the death numbers will likely be 10x that
You can't have your cake (150k deaths) and eat it too (widespread)
But if we allow exponential growth on a high base, if allow high proportion of general population to become infected, the death numbers will likely be 10x that
You can't have your cake (150k deaths) and eat it too (widespread)
12/ In NYC (20% cum incidence) CONFIRMED death rate from COVID so FAR for 45-64 yo age group is ~180 per 100k pop
We know that's an under-estimate, and we still have a lot of deaths yet to come->closer to 360/100k
At national scale that would mean 290,000 deaths JUST IN 46-64yo
We know that's an under-estimate, and we still have a lot of deaths yet to come->closer to 360/100k
At national scale that would mean 290,000 deaths JUST IN 46-64yo
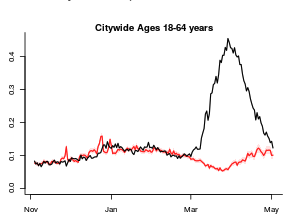
13/ And the focus on lower DEATH rate among those <65 is also incomplete
Fully HALF of all hospitalizations in NYC were among those <65.
Even at the 20% infection level, there was an astounding level of ER visits among younger groups. The bump on left was flu
HT @WeinbergerDan
Fully HALF of all hospitalizations in NYC were among those <65.
Even at the 20% infection level, there was an astounding level of ER visits among younger groups. The bump on left was flu
HT @WeinbergerDan
14/ WE CAN'T ALLOW EXPONENTIAL GROWTH ON A HIGH BASE in any age group.
And while the @freopp authors are laudably calling for much greater attention to nursing home deaths- it will be VERY VERY hard to protect 100M old/vulnerable in the midst of a raging pandemic.
And while the @freopp authors are laudably calling for much greater attention to nursing home deaths- it will be VERY VERY hard to protect 100M old/vulnerable in the midst of a raging pandemic.
15/ Who will take care of the old and the vulnerable?
How do we think we can protect them from asymptomatic and presymptomatic caretakers? How effectively can we control outbreaks in congregate settings?
We HAVE TO keep infection rates down in the general population
How do we think we can protect them from asymptomatic and presymptomatic caretakers? How effectively can we control outbreaks in congregate settings?
We HAVE TO keep infection rates down in the general population
16/ >40% of all deaths in the US are in nursing homes and long-term care facilities- this is a huge problem, and there should be a lot more attention to detection and mitigation and infection control.
But plans to segregate the old from the young don't seem to work.
Sweden.
But plans to segregate the old from the young don't seem to work.
Sweden.
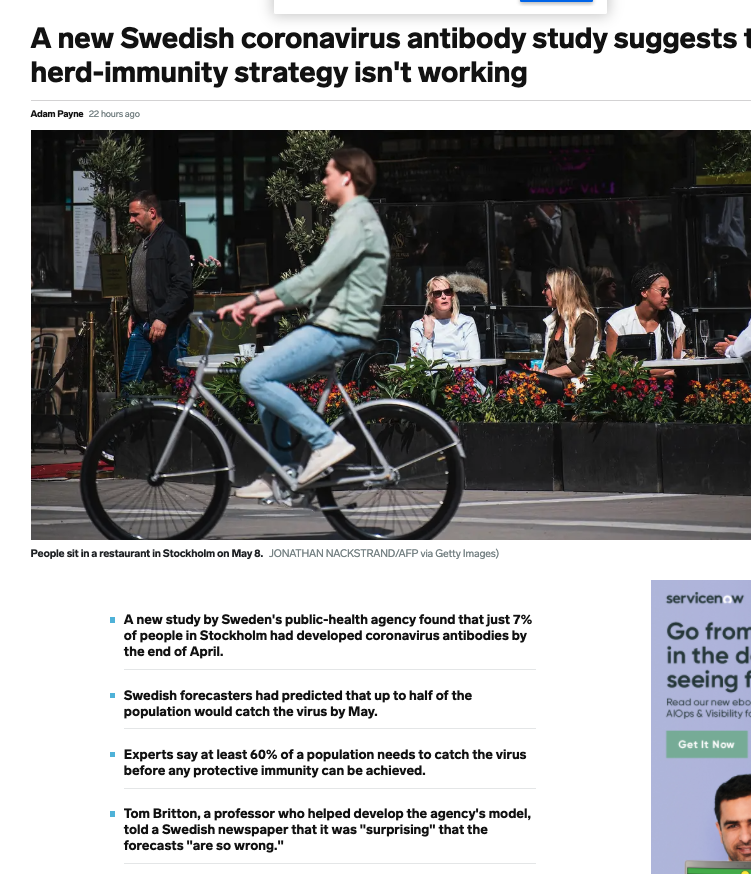
17/ I am glad they tried to do something different, and we need to wait for more data, but 49% of deaths there have been in care homes.
This does not bode well for our ability to protect the elderly
And I don't know when herd immunity might kick in, but doesn't seem close by
This does not bode well for our ability to protect the elderly
And I don't know when herd immunity might kick in, but doesn't seem close by
18/ Sweden's social structure is quite different from ours w 56% in single person HH (vs 27% in US)
And they DID implement a lot of social distancing (on Facebook mobility they were on par with Alabama), and official projections are for GDP contraction by 7-10% (on par w EU 7%)
And they DID implement a lot of social distancing (on Facebook mobility they were on par with Alabama), and official projections are for GDP contraction by 7-10% (on par w EU 7%)
19/ BTW- I hear a lot about how we should discount the experience of the largest outbreak epicenter we have experience with, the NY metro area.
NY may be different in density, subway, etc that fanned the flames of outbreak spread, but that won't affect the % symptomatic/ IFR
NY may be different in density, subway, etc that fanned the flames of outbreak spread, but that won't affect the % symptomatic/ IFR
20/ If your policy capitulates that we will eventually have 20%-50% of the population infected - the same number of people will get sick, will die.
Even a smoldering rolling outbreak with one to two thousand deaths a day- that we are somehow getting inured to- is a catastrophe
Even a smoldering rolling outbreak with one to two thousand deaths a day- that we are somehow getting inured to- is a catastrophe
21/ It's possible that reopening "blind" will not cause immediate NY/NJ/CT/MA/New Orleans/Detroit-like outbreaks. I hope so
People and businesses will continue to be careful, the weather is getting warmer/more humid.
We may get lucky.
But why not get "eyes" on it first?
People and businesses will continue to be careful, the weather is getting warmer/more humid.
We may get lucky.
But why not get "eyes" on it first?
22/ So back to you, @Avik @lanheechen
Would you reopen if it could mean exponential growth on a high base of active infections?
Without gating criteria can you be confident of that?
What level of cumulative infections would be OK among those < 65?
Can we segregate elderly?
Would you reopen if it could mean exponential growth on a high base of active infections?
Without gating criteria can you be confident of that?
What level of cumulative infections would be OK among those < 65?
Can we segregate elderly?

23/ We CAN'T be confident w/out gating criteria
If you reopen w lots of active infections & R>1, then reopening- however mitigated-WILL increase R, set us up for exponential growth
W/out surveillance, have 50X increase by the time you see deaths spike
🤷♂️
If you reopen w lots of active infections & R>1, then reopening- however mitigated-WILL increase R, set us up for exponential growth
W/out surveillance, have 50X increase by the time you see deaths spike
🤷♂️