
1/ Our latest work was just published in @NatureMedicine!
Congratulations to first author Super-Star @BraunMDPhD and to all authors. #CathyWu #SachetShukla @LabSignoretti @VanAllenLab #FreemanLab #SharpeLab
@DanaFarberNews @DanaFarber
#kcsm #KidneyCancer
doi.org/10.1038/s41591…
Congratulations to first author Super-Star @BraunMDPhD and to all authors. #CathyWu #SachetShukla @LabSignoretti @VanAllenLab #FreemanLab #SharpeLab
@DanaFarberNews @DanaFarber
#kcsm #KidneyCancer
doi.org/10.1038/s41591…
2/ Our study analyzes patient samples from 3 prospective clinical trials of PD-1 blockade.
The study includes 592 tumors that were profiled by WES, RNA-seq, and/or IF for CD8+ T cells on samples collected before treatment with Nivolumab (anti-PD1) or Everolimus (mTOR inhibitor)
The study includes 592 tumors that were profiled by WES, RNA-seq, and/or IF for CD8+ T cells on samples collected before treatment with Nivolumab (anti-PD1) or Everolimus (mTOR inhibitor)
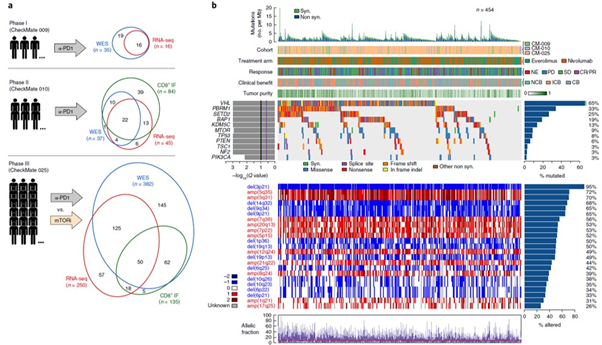
3/ We evaluated genomic correlates of response to PD-1 inhibitors in ccRCC.
Molecular features that had been previously suggested to correlate with outcomes (e.g. TMB, NeoAg load) were not found to be predictive of benefit from PD-1 blockade.
Molecular features that had been previously suggested to correlate with outcomes (e.g. TMB, NeoAg load) were not found to be predictive of benefit from PD-1 blockade.


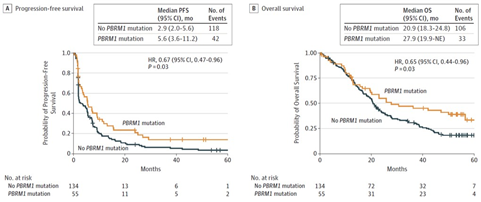
4/ PBRM1 truncating mutations were the only significantly recurrent mutations that were found to correlate with outcomes with nivo (but not observed with everolimus).
Crucially, patients had largely received Nivo in 2nd line or beyond (after VEGF TKI).
Crucially, patients had largely received Nivo in 2nd line or beyond (after VEGF TKI).


5/ This finding in the present pooled analysis builds on our initial work with @VanAllenLab @kaelinLab published in @ScienceMagazine and our prior validation study with @BraunMDPhD in @JAMAOnc.
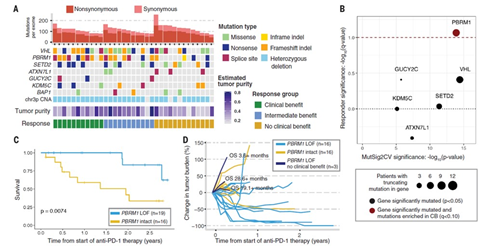
6/ We then used CD8+ IF and spatial analysis to evaluate the patterns of immune infiltration in ccRCC.
We found that most tumors are immune infiltrated, with few immune desert/excluded tumors. However, the pattern of immune infiltration was not predictive of outcomes with Nivo.
We found that most tumors are immune infiltrated, with few immune desert/excluded tumors. However, the pattern of immune infiltration was not predictive of outcomes with Nivo.



7/ With relatively little predictive value in individual genomic or immune features, we next evaluated the potential interplay between genomic features and the immune infiltrate.
We found that PBRM1 mutations are enriched in immune excluded/desert tumors.
We found that PBRM1 mutations are enriched in immune excluded/desert tumors.

8/ Conversely, we found that multiple somatic copy number alterations are significantly enriched in infiltrated tumors.
Among these alterations, only 9p21.3 deletions were associated with poor survival (with Nivo but not observed with Everolimus).
Among these alterations, only 9p21.3 deletions were associated with poor survival (with Nivo but not observed with Everolimus).



9/ Overall, the findings of our study suggested a possible interplay between genomic/immune features in ccRCC, whereby non-infiltrated tumors (CD8+T cell low) that may otherwise be less likely to respond to Nivo, are enriched in PBRM1 mut that increase their chance of response.

10/ By contrast, tumors that are infiltrated with CD8+ T cells may be poised to respond to Nivo, but the significant enrichment in clinically unfavorable 9p21.3 deletions (the locus for CDKN2A/B) in these tumors correlates with poor outcomes on Nivo.

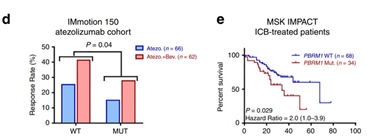
11/ A special note on PBRM1 mutations and outcomes on ICI: Our own prior @ScienceMagazine study and subsequent work from #IMmotion150 in @NatureMedicine suggest that the correlation between these mutations and outcomes differs by treatment setting. Please do not ignore that fact!
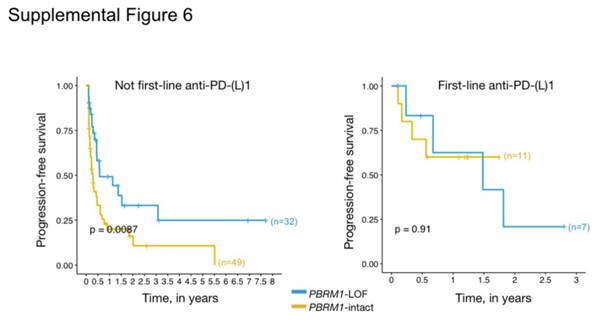

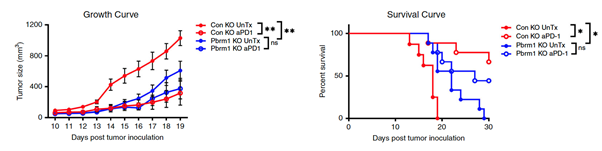
12/recent @NatureComms paper re-analyzed data from FIRST Line #IMmotion150 &showed that PBRM1 correlates with PD1 "resistance". However, using RENCA model (not a ccRCC VHL null model!), PBRM1 KO lines grow at same rate as PD1-treated lines! ==>Complex IFN signaling?
13/ This clinical finding is again consistent with the suggestion that PBRM1 mutations do not have the same predictive value in the 1st line setting. Prior anti-angio Tx may play a crucial role in "priming" the immune TME, although this requires further study.
14/Again: biologically relevant vs. a predictive biomarker (in a very specific clinical context) =2 very different things and it is incorrect if you see the former to assume the latter, as some are doing.
15/ Some studies in this setting are supportive:
•@sarahAbouAlaiwi, @CIR 2020 cancerimmunolres.aacrjournals.org/content/early/…: Oncopanel data: SWF/SNF alternations have no effect on IO outcomes. Exceptions: RCC: association with TTF, OS
•@sarahAbouAlaiwi, @CIR 2020 cancerimmunolres.aacrjournals.org/content/early/…: Oncopanel data: SWF/SNF alternations have no effect on IO outcomes. Exceptions: RCC: association with TTF, OS
16/ Other studies:
•Vano, ASCO GU 2020, HR OS 0.59 in PBRM1 loss by IHC (France), @LAlbiges
•City of Hope, AACR 2020 (HR<1, in CB pts, p=0.2) @montypal @NazliDizman (small cohort)
•Vano, ASCO GU 2020, HR OS 0.59 in PBRM1 loss by IHC (France), @LAlbiges
•City of Hope, AACR 2020 (HR<1, in CB pts, p=0.2) @montypal @NazliDizman (small cohort)
17/ The overall evidence to date and the findings of our study therefore suggest that ccRCC is characterized by a distinctive interplay between tumor genomic features and the immune microenvironment. Further study of the effect of systemic therapy (+anti-angio) is needed!

