1/Which fluid is more appropriate in patients with hyperkalaemia 0.9% saline or Hartmann’s?
A #pedsicu thread:
How much K+ does Hartmann’s solution and 0.9% Saline solution contain respectively ?
A #pedsicu thread:
How much K+ does Hartmann’s solution and 0.9% Saline solution contain respectively ?
2/ Hartmann’s solution has 4mmo/L of K+
0.9% saline has no K+ content.
So with that in mind, which one do you think is safer to use in a patient with hyperkalaemia (lets assume that's someone with a K+ more ore equal to 5.5mmol/L)
0.9% saline has no K+ content.
So with that in mind, which one do you think is safer to use in a patient with hyperkalaemia (lets assume that's someone with a K+ more ore equal to 5.5mmol/L)
3/
There is a very common misconception that Hartmann’s solution(aka) Ringer’s lactate is contraindicated in patients with hyperkalaemia. We are challenged on this almost weekly when we get pedicu referrals @NWTStransport
There is a very common misconception that Hartmann’s solution(aka) Ringer’s lactate is contraindicated in patients with hyperkalaemia. We are challenged on this almost weekly when we get pedicu referrals @NWTStransport
4/There is a grand total of zero evidence that ringer’s lactate exacerbates hyperkalaemia. So why does have this firmly held belief persist and why is it wrong. There are 3 reasons to this:
5/How much of total body potassium is intracellular and what is its concentration ( roughly)
6/ Reason 1:
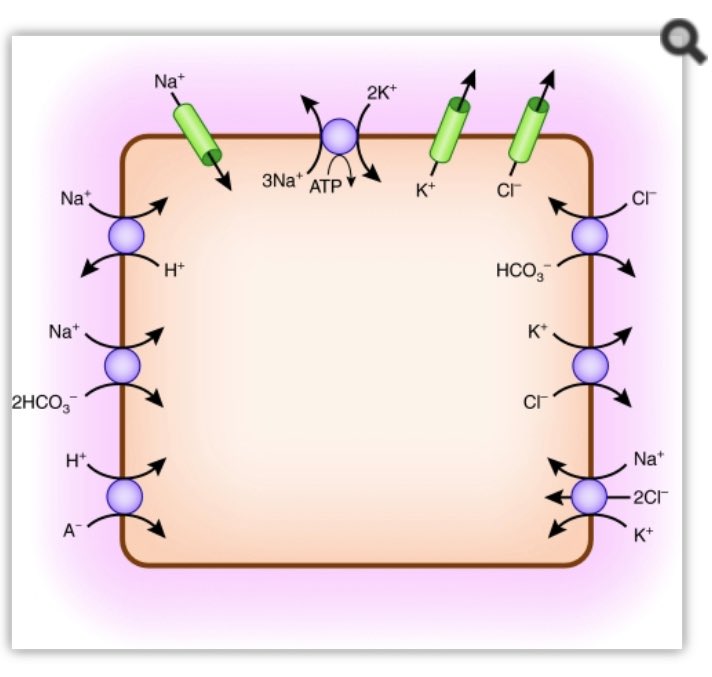
The bulk of total body potassium is intracellular (about 98%) with a concentration of roughly 140mmol/L. Even a minute shift from within the cell to the extracellular environment can have a dramatic rise on extracellural K+ concentration. (Ab)normal saline is
The bulk of total body potassium is intracellular (about 98%) with a concentration of roughly 140mmol/L. Even a minute shift from within the cell to the extracellular environment can have a dramatic rise on extracellural K+ concentration. (Ab)normal saline is
7/Chloride rich and sudden flux of chloride causes hyperchloraemia with resulting non-anion gap metabolic acidosis. Much like sodium bicarbonate (a base) is used in many hyperkalaemia protocols in order to alkalinise the extracellular environment and drive K+ to the intracellular
8/compartment, the reverse happens when we acidify our patients by giving choride rich solutions. The acidosis caused by causes a K+ shift from inside the cell to the exctracellural compartment causing a hyperkalaemia. Hartmann’s on the other hand is a weak base as it contains
9/ 28mmol/L of HCO3- physiologically it is more likely to cause a K+ shift in the opposite direction.
If you are interested in the intricacies of K+ homeostasis at a cellular level in response to pH I would highly recommend this paper by Aronson et al bit.ly/2TUUy49
If you are interested in the intricacies of K+ homeostasis at a cellular level in response to pH I would highly recommend this paper by Aronson et al bit.ly/2TUUy49
10/ If, at standard conditions, you have two solutions of equal volume ( say 500ml each) one having a K+ concentrayion of 10 mmol/L and one with a concentrayion of 4mmol/L , what will be then net K+ concentraion if you mix the two together to make a litre of solution.
11/ Reason 2: If we are having the conversation whether Hartmann’s will exacerbate your patient’s hyperkalaemia or not, it is safe to assume that your patient has a high enough K+ levels for you to worry about them (lets say 5.5mmol/L or above). As we established earlier
12/ Hartmann’s has 4mmol/L of K+ in , significantly lower than the patient’s potassium concentration . Mixing a more dilute solution with a more concentrated solution can never make the net solution more concentrated; it can only make it less concentrated.
13/Reason 3:
The distribution volume of K is far greater than the extracellular fluid volume. Any infusion with a physiologically appropriate K+ concentration will have minimal influence on serum K+ levels. Take a 50kg teenager for example. Assume our patient’s K+ =7mmol/L
The distribution volume of K is far greater than the extracellular fluid volume. Any infusion with a physiologically appropriate K+ concentration will have minimal influence on serum K+ levels. Take a 50kg teenager for example. Assume our patient’s K+ =7mmol/L
14/
What is the estimated total Extracellular fluid of our patient ( ECF is plasma plus Interstitial fluid plus transcellular fluid)
What is the estimated total Extracellular fluid of our patient ( ECF is plasma plus Interstitial fluid plus transcellular fluid)
15/ The ECF volume is 10 litres roughly (plasma volume is 2.5L,interstitial fluid volume 7.5 litres whilst intracellular fluid is 20 litres)
Now imagine we give him/her a litre of a theoretical solution containing 9 mmo/L of K+(remember this is a thought experiment don’t try irl)
Now imagine we give him/her a litre of a theoretical solution containing 9 mmo/L of K+(remember this is a thought experiment don’t try irl)
16/ Post infusion, the K+ should be a weighted average of the two solutions mixed together. What is the net concentration after the infusion?
17/ 7mmol/L x 10 litres and 9 mmol x 1 litre gives us a net concentration of 7.18 mmol/L . A measurable difference of 0.18mmol/L but a very small one. Add into the calculation that potassium balances continuously between the intracellular and extracellurar space , the volume of
18/ distribution is much higher than the ECF thus our net K+ increase will be lower than 0.18mmo/L. Now remember that our thought experiment was done with a solution with more than double the K+ concentration of Hartmann’s , and we found that in theory it would increase the serum
19/ K+ by less than 0.18mmol/L we would need much more volume for such fluid to cause a significant potassium rise. So the theory may be convinving but do you have any evidence?
Funny you should mention it, there are at least 3 papers I could find ,
Funny you should mention it, there are at least 3 papers I could find ,
20/ all of which are prospective double-blind randomized controlled trials These compare the effect of Hartmann’s solution VS (ab)normal saline on the potassium levels in patients with renal failure.
The 1st study was published by O’Malley and colleagues
pubmed.ncbi.nlm.nih.gov/15845718/
The 1st study was published by O’Malley and colleagues
pubmed.ncbi.nlm.nih.gov/15845718/
21/ A prospective double blind RCT when the two fluids were used intraoperatively in adult patients undergoing renal transplants. Primary outcome was postop creatinine levels. 51 patients in, the study was stopped due to safety concerns as interim analysis showed that in the
22/ 0.9% Saline group 19% developed K+> 6 and 31% developed metabolic acidosis requiring bicarb correction. None of the patients receiving Hartmann’s developed hyperkalaemia or acidosis requiring correction ( p = 0.05 and 0.004 respectively)
23/ Khajavi repeated the study (almost identical )52 patients undergoing renal transplant. The mean change in serum potassium during the procedure was +0.5 mmol/L in the (Ab)normal saline group compared to -0.5 mmol/L in the Hartmann’s group (p < 0.001)bit.ly/3gHnE0C
24/The largest study n=74was by Modi ( only published as a letter to editor). Again, this was almost identical to the two above. K+ increased in the saline arm group by 0.37 mmoL/L (p < 0.05). There was no significant change in K+ in the Hartmann’s arm
shorturl.at/jF478
shorturl.at/jF478
25/ Study limitations:
Don't factor in intraoperative K+ surge due to tissue damage/ apoptosis . Also the volumes given in the studies are very liberal, it is likely that smaller infused volume will cause less dramatic swings in K and pH.
Don't factor in intraoperative K+ surge due to tissue damage/ apoptosis . Also the volumes given in the studies are very liberal, it is likely that smaller infused volume will cause less dramatic swings in K and pH.
26/ In Summary Hartmann’s is not only , not contraindicated as a fluid choice in patients with hyperkalaemia, but it is a safer option than (ab)normal saline . /end