
I’ve been seeing a lot of conflicting information about tear gas online and wanted to make a guide about what tear gas is, how it’s used and how to treat exposure to it. I have a background in experimental methodology and research, and am an amateur chemist.
Special thanks to @3liza for this thread that gave me inroads to the literature, @taliabear for proofreading this and my professional chemist friend who wishes to remain anonymous for reviewing this.
So the first thing to really drive home: Tear gas isn’t just one thing. There’s nearly a dozen different compounds that are used as riot control agents across the world. I’ll be focusing on the USA because that’s where I live.
These are the most common compounds used as tear gas in the USA, roughly in order of prevalence of use:
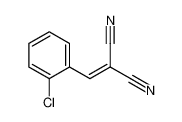
[(2-Chlorophenyl)methylidene]propanedinitrile (CS)
Oleoresin Capsicum (OC)
2-chloro-1-phenylethanone (CN)
Ironically none are gases at standard pressure and temperature.
[(2-Chlorophenyl)methylidene]propanedinitrile (CS)
Oleoresin Capsicum (OC)
2-chloro-1-phenylethanone (CN)
Ironically none are gases at standard pressure and temperature.
All three of these compounds can be used individually or together and manufacturers make combo canisters that can dispense multiple at once, which is part of what makes treatment difficult: It’s hard to know exactly what compound(s) someone has been exposed to. 
CS is by far the most common and is probably what comes to mind when you hear the word “teargas”. It’s insoluble in water, which is important for later, and is dispersed as an aerosol either by burning into smoke (most common for riot control) or mixed in a solvent as a spray.
Dealing with CS canisters is straightforward: Containing the smoke before it spreads and dousing the fire is the most efficient way to prevent widespread dispersal of CS. Remember that these canisters are literally on fire, burning noxious chemicals.
CS works by coming in contact with mucus membranes and activating the TRPA1 ion channel (1). This is the same general chemical pathway that produces horseradish’s burning sensation on the tongue. It’s electrophilic and is likely to react with anything that is wet.
CS is active in very small amounts, with research (2) reporting people having adverse reactions to as little as 5 mg of CS per square meter air. It’s important to wash everything exposed to CS thoroughly, as it can and will irritate you and others around you over time.
Precautions you want to take if you think you’ll run into CS: Cover yourself up to prevent CS from sticking directly to your skin and hair, wear goggles to limit contact with eyes, and a mask. No seriously: between all of these, COVID-19 and persistent surveillance wear a mask.
You may have seen people covering themselves in plastic wrap. Taking the Roy Orbison approach can be effective but has drawbacks. It keeps CS off your skin and can be unwrapped and thrown away making decontamination easier.
However, it doesn't breathe, it can cause overheating and is just plain uncomfortable which isn't great for protesting morale. It's a reasonable emergency "Oh hey I just woke up and there is a cloud of CS outside my door" kinda thing.
A few things not to do as well: don’t wear makeup, as it can attract the electrophilic CS particles and trap it in a harder to remove base. Also don't wear eye contacts as CS particles can get trapped between contacts and your eye making it much harder to deal with.
In addition, both contacts and makeup encourage you to touch your face more, which is something to be mindful of at protests: Even if you haven’t been directly hit, cross contamination is very possible and touching something covered in CS then touching your face is a bad time.
Treatment for CS exposure is pretty straightforward in one way: Get out of the area with CS and don’t touch your face and wash it off. This prevents you from accidentally applying more CS to yourself and prevents you from accidentally hurting yourself.
Treating pain is trickier. Since CS isn’t soluble in water, flushing with water/saline can spread CS and cause more pain before getting better. Using forced hot air appears better (3,4) and has been adopted by the UK (5) but may not be practical in a protest.
Most medical orgs (6,7, 9) recommend high volume irrigation with water for at least 10 minutes, as the primary treatment for exposure to CS. It is the most practical treatment even if it causes more pain in the short term, by preventing long term eye damage via crystallization.
CS does hydrolyse rapidly and does so in basic conditions faster than neutral ones (2), so there may be truth to using liquid antacid/water (LAW) to treat CS being effective, but no research has been done on CS and basic solutions for efficiency.
Do not use baking soda or solid antacids as these can be abrasive and make things worse. Milk is right out, there’s no properties of milk that would be useful in dealing with CS. Baby shampoo was found to be ineffective for CS and OC (12).
Another complicating factor when dealing with CS is that chemical weapons manufacturers keep “improving” it in various ways. CS2 for example adds a silicone based water repellent to the mix that makes it harder to wash out. (5)
Chemical weapon manufacturers don’t have to label all the ingredients in their weapons and modifications on this seem to be trade secrets. How these chemicals react under heat, with other products in concurrent use, is a witch’s brew and very few studies have looked into it.
Next I’m going to talk about CN as chemically, it's a close cousin to CS. This used to be the most common form of tear gas used across the world until the 1980s due to research coming out showing how much more toxic CN compared to CS. (8)
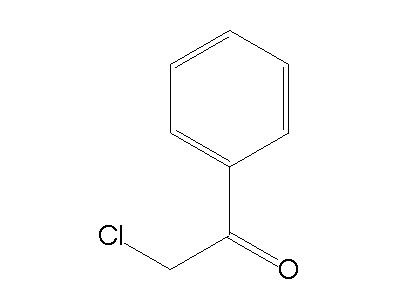
CN is still the main component of brand name Chemical Mace (Yes, mace is a trademark that became genericized) and is used when more physical deterrence is needed than CS or OC. It has a slower onset and requires more contact than either CS or OC to function. (9)
CN is mostly used as a spray, carried in a solvent but some companies still make pyrotechnic canisters like the ones used for CS, along with fogging/spraying style grenades similar to OC products.
CN uses the same pathway as CS, the TRPA1 ion channel, so CS and CN fight over the same receptor sites, but have a few notable differences. CN is way more likely to cause pain and blistering on the skin than CS (9).
Because a larger effective dose is needed and CN has a longer onset it’s not as useful for dispersing crowds, but it is more effective for incapaciting individuals because of its intensity and duration, which are significantly longer. (9)
Functionally, prevention and treatment are the same for CN as CS (9). Avoidance of skin exposure is more important due to CN’s blistering effects, but treatment is the same: Leave the area, wash exposed areas, forced hot air or water flushing for the eyes.
Significantly less research has been done into CN as it was phased out of large scale use before the more recent boom in literature on tear gas. More research has been done in the last six years on teargas than the preceding 40 years.
And finally we have OC. If you see a pepper-X product, it is very likely based on OC, which is a solvent extraction of organic wax in chili peppers with high levels of capsaicin. There is also PAVA which is a synthetic capsaicinoid powder with the same path of action.
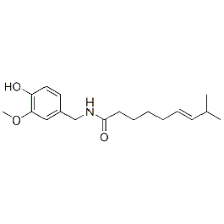
OC is technically a mix of a bunch of organic compounds since it is an extract from a natural product. While capsaicin is the primary agent, there’s a whole family of capsaicinoids including PAVA in the mix. As a wax, OC is almost always dissolved in a solvent.
OC is most commonly dispersed in spray form, but also can exist as paintballs, spray grenades, and other carrier liquids. PAVA is a powder and is used as condensed balls, bullets, or packed into powder grenades.
OC/PAVA works by activating a different ion channel than CS does, TRPV1. This means that if you get exposed to CS and OC at the same time, both will burn and irritate you in different ways and have some synergistic effects, which is why they are often used together.
Everything I said about precautions about CS are reasonable precautions for OC as well, though there’s one major difference: masks: Droplet sizes for OC products are 2-120 microns and vary quite a bit between product, distance and how much OC is left (10).
That means that a wider range of masks are going to be more useful at stopping OC than CS because the particles on average are at least twice and at most, several orders of magnitude larger. Any mask is better than no mask and this is even more true with OC.
Treatment has some similarities to CS treatment: removing people from exposure and washing everything that’s come in contact with it is still the best first step. People are even more sensitive to OC than CS in general (9) so it really pays to be thorough here.
OC is a wax dissolved in alcohol, so water is less effective on it than CS, with most sources recommending streaming water for 15-20 minutes for exposure (9,11,12,13,14) unlike the briefer CS treatment. It is still the best treatment for preventing long term eye damage(12).
LAW, Milk, Lidocaine, Baby Shampoo have all been tested as treatments for OC and none of them have shown to be effective in clinical trials (12,14) though LAW had more success when applied without eye exposure (15) but the trial is tiny.
No formal research on forced hot air has been done for OC exposure, but anecdotal evidence (16) suggests it may be effective. I made a request for the literature reference mentioned as the basis for testing a hairdryer to the posted email address but got no response.
One special note: If you’re a tampon user, be very careful with carrying them to protests and using them. During this research I found a case study (17) in which a lady used an OC contaminated tampon and 4mg of morphine didn’t help with the pain.
While editing this piece, the chemist I worked with related a time where they were exposed to a small amount of a chemically similar compound to CS via a triple washed vial, through a ventilated hood, five meters away.
Even with all reasonable precaution and a controlled environment, exposure happens. This was a minimal amount of a less reactive substance through multiple protective pieces of equipment and was still incapacitating and needed a 15 minute stint in the eye wash station.
So if one thing you take away from all this, the TLDR is: The most agreed upon course of treatment for exposure to any of the teargases is to get out and wash up with water. Forced hot air might be worth a deeper look at, LAW has some conflicted support. Everything else is bunk.
Works Cited (cont)
5. nature.com/articles/eye19…
6. emergency.cdc.gov/agent/riotcont…
7. who.int/csr/delibepide…
5. nature.com/articles/eye19…
6. emergency.cdc.gov/agent/riotcont…
7. who.int/csr/delibepide…
Works Cited (cont)
8. link.springer.com/article/10.100…
9. militaryhealth.bmj.com/content/jramc/…
10.govinfo.gov/content/pkg/GO…
8. link.springer.com/article/10.100…
9. militaryhealth.bmj.com/content/jramc/…
10.govinfo.gov/content/pkg/GO…
Works Cited (cont)
11 hkmj.org/abstracts/v21n…
12 ncbi.nlm.nih.gov/pmc/articles/P…
13 bmj.com/content/bmj/33…
11 hkmj.org/abstracts/v21n…
12 ncbi.nlm.nih.gov/pmc/articles/P…
13 bmj.com/content/bmj/33…
Works Cited (cont)
14 web.archive.org/web/2018071911…
15 onlinelibrary.wiley.com/doi/epdf/10.11…
16 medic.wikia.org/wiki/OC_trials
14 web.archive.org/web/2018071911…
15 onlinelibrary.wiley.com/doi/epdf/10.11…
16 medic.wikia.org/wiki/OC_trials
Works Cited (end)
17 ncbi.nlm.nih.gov/pmc/articles/P…
17 ncbi.nlm.nih.gov/pmc/articles/P…

