
Protestors&others: A negative test for COVID-19 does NOT RULE OUT INFECTION if you don't have symptoms (& it's not 100% accurate even if you do). Let me explain 1 of the giant unknowns for testing for COVID-19/SARS-COV-2 that impacts so many things. Discussed w/ @CT_Bergstrom
What we DO know: a very nice synthesis by @bennyborremans of testing of people for RNA suggests that upper respiratory tract swabs (purple line/points) are >90% accurate in identifying people who are infected during the 1st 5 days AFTER symptom onset. medrxiv.org/content/10.110… 
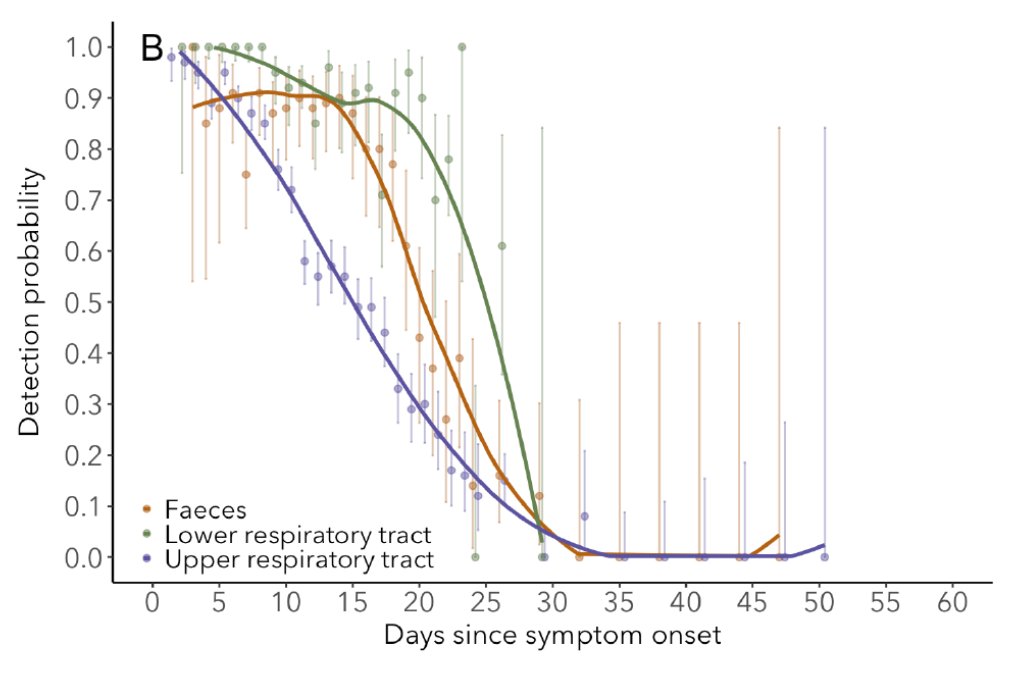
The problem is that there are NO data (none!) BEFORE symptom onset, so we have NO IDEA if a negative swab test provides solid evidence you are uninfected, or no information at all if you don't have symptoms. All data are from people that already have symptoms!
Some of you might have seen this paper/figure that supposedly had data on this key question. It actually doesn't. It has data from a single person (N=1) swabbed several times, but this person NEVER tested positive by swab (only endotracheal aspirate).
acpjournals.org/doi/10.7326/M2…
acpjournals.org/doi/10.7326/M2…
Thus, that patient tells us nothing about when a person will test positive by swab for people that eventually do. Many other issues too. (For those that want to go down the rabbit hole, the N=1 patient is #13 in Fig 4 from this paper:
academic.oup.com/cid/advance-ar…).
academic.oup.com/cid/advance-ar…).
Many of you might say: Wait! I know of tons of examples of people testing + without or before symptom onset. Yes! You are right. But none of those reports/studies show data from people over time to determine when, after infection, but before symptoms, they start testing positive.
And some never develop symptoms at all (actual fraction is uncertain - see ). For these people we also have no idea when, post-infection, or with what probability, truly asymptomatic people test + or their viral loads over time.
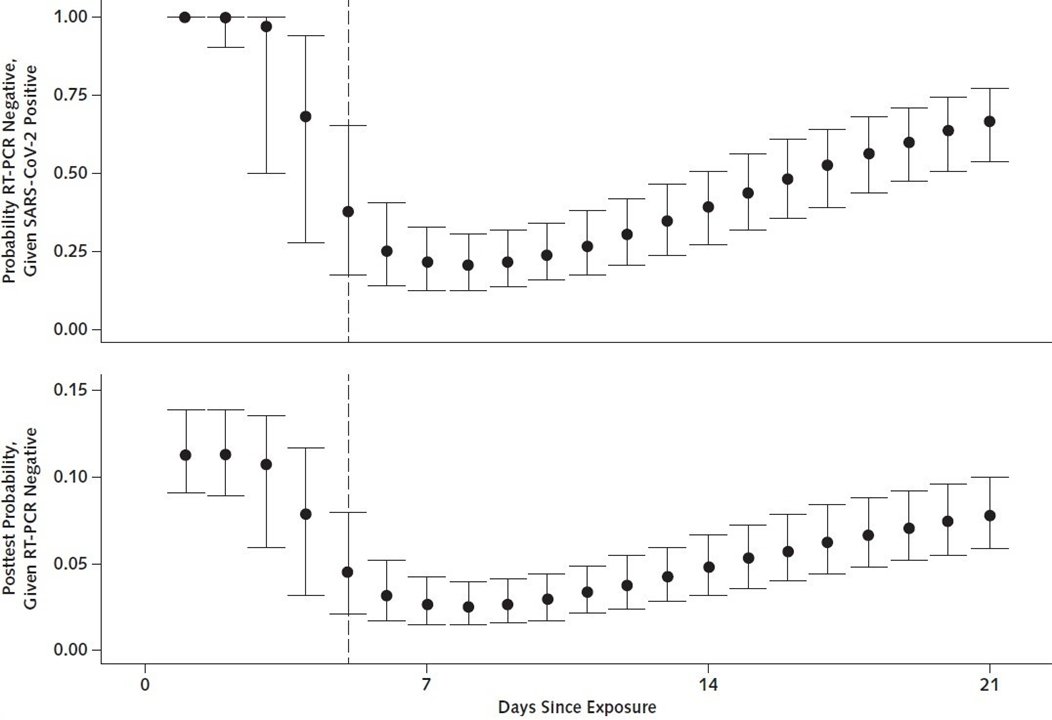
Without data on how accurate pre-symptom onset testing is ("sensitivity" is the technical term for 1-prob of false negative; most PCR tests are thought to be very "specific" - i.e. there are very few false positives), standard protocol is to isolate yourself for 14 days.
Why 14d? Because symptoms show up within ~14d for 95% of people that do become sick and if you get sick you go & get tested (and then results above apply). Also, hopefully, if you're sick you continue to isolate regardless of test!
So why does this matter? So many reasons! It affects protests, tourism, travel, business operation, schools. Everything really! I'll explain.
Protests: Following protests (or any risky contact), people are getting tested for COVID-19/SARS-COV-2. If you test negative does that mean you can be CONFIDENT that you are not infected and can safely see family or go protest more? NO. You could be infecting them (be careful!).
Tourism: Did you hear NZ is COVID-free? Amazingly, yes! How are they going to keep it that way? By testing incoming asymptomatic passengers? Nope! We don't know what fraction of infected people it would identify. See reasons above. You will have to quarantine/isolate for 14 days.
Business travel to place X (e.g. UK, Hong Kong): Want to do a 2 day business trip to UK, Hong Kong and feel fine? No problem right? Just get tested when you land? Nope. See above. Need to quarantine/isolate for 14 days. Suddenly a 2 day business trip is a 16 day trip.
Business operation: One of your employees tests + for COVID. Yikes! Have to shut down the whole business? Can't you just test all your asymptomatic employees and if negative go back to work? Nope. See above. All close contacts will need to quarantine/isolate for 14 days.
Business operation follow up: This lack of ability to rule out infection should create huge incentive for businesses to provide employees with safe working conditions (1-2m space, requiring masks, adequate ventilation, etc) so they aren't close contacts.
Schools: Want to re-open schools/Univs but don't want to start year off with a COVID epidemic? No problem, just screen all the asymptomatic incoming students right? Nope. See above. All students would need to quarantine/isolate for 14 days. Quarantining 1000s of students? Yikes!
Hopefully I've convinced you this is a GIANT issue.
Luckily it's actually pretty simple to collect the data to answer this question and I'm shocked it hasn't been done yet. (In fact someone may have the data already and just needs to share it. If you do please do!) How to do it:
Luckily it's actually pretty simple to collect the data to answer this question and I'm shocked it hasn't been done yet. (In fact someone may have the data already and just needs to share it. If you do please do!) How to do it:
When you detect a case, find their RECENT close contacts and start swabbing them immediately. Most valuable would be contacts from the last 1-2 days. Swab them 1st day and every day for the next 14+ days and test by PCR. Record symptoms daily. Repeat. It's that simple
Even with a limited sample size this would provide extremely valuable info on 2 things that are unknown:
1) test sensitivity vs day of infection and days before symptom onset as detailed above
2) viral load vs infection and days before symptom onset to estimate infectiousness
1) test sensitivity vs day of infection and days before symptom onset as detailed above
2) viral load vs infection and days before symptom onset to estimate infectiousness
Infectiousness vs days since infection BEFORE symptom onset is also, amazingly, unknown. The closest we have is estimates from actual transmission events, not viral load. The best example I know of is based on avg data that I've redrawn (from Fig 1C of nature.com/articles/s4159…):
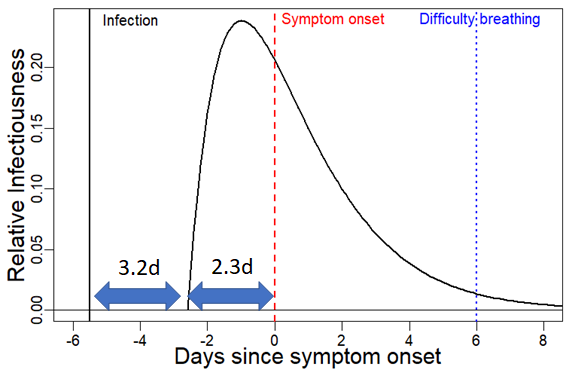
But b/c it's based on transmission events not viral load, it confounds infectiousness and contact rates. It suggests that infectiousness is high (and higher actually) before symptom onset than after. Many studies suggest pre- or asymptomatic transmission is ~50% of transmission.
It's possible infected people would test + by swab when they are heavily infectious (days 2.5-0 pre-onset), & possibly even in days before that. That would be great! But we don't know! If they don't, that will make frequent testing far less effective for reducing transmission.
The graph above shows data for average person (incubation 5.5d) but even more important data would be from people who get symptoms on days 10-14. Are these people infectious for many days before they get symptoms or just 2-3? Would they test +? When? Huge questions!
If testing can be used to identify infected people before they are symptomatic & ideally before they are infectious this could change everything I listed above - protesting, travel, business, schools. It could also shorten quarantining from 14d to ?? We need this data!
I'd appreciate anyone working in public health doing contact tracing who could collect these data to do so and share ASAP.
(Note: If possible (it's hard, I know), INFECTIOUS viral load from cell culture would be much more valuable than just RNA via PCR)
(Note: If possible (it's hard, I know), INFECTIOUS viral load from cell culture would be much more valuable than just RNA via PCR)
Worth noting that low viral load just after infection means testing is more likely to miss infection earlier than later. But exact time course of viral load vs days since infection unknown!


