A follow-up to recent monster #HematologyTweetstory 22 on the names of all 71 @theNCI Cancer Centers: the National Comprehensive Cancer Network (@NCCN), which (especially outside the US) is sometimes confused w/ @theNCI, but doesn't get direct NCI funds./1 nccn.org/members/networ…
@NCCN was a mystery to me as a hematology-oncology fellow. What is it, exactly? A cancer center faculty club?🙂A quasi-cooperative group? I suspect I wasn't alone in my confusion. This thread will include some history & description - and will mention a few areas of controversy./2 



The other 4 compendia: @ElsevierConnect Gold Standard’s Clinical Pharmacology; @ASHPOfficial
American Hospital Formulary Service Drug Information (AHFS-DI®); @thomsonreuters Micromedex DrugDex®; @Wolters_Kluwer Lexi-Drugs®. These are useful, too, but aren't heme-onc specific./5
American Hospital Formulary Service Drug Information (AHFS-DI®); @thomsonreuters Micromedex DrugDex®; @Wolters_Kluwer Lexi-Drugs®. These are useful, too, but aren't heme-onc specific./5
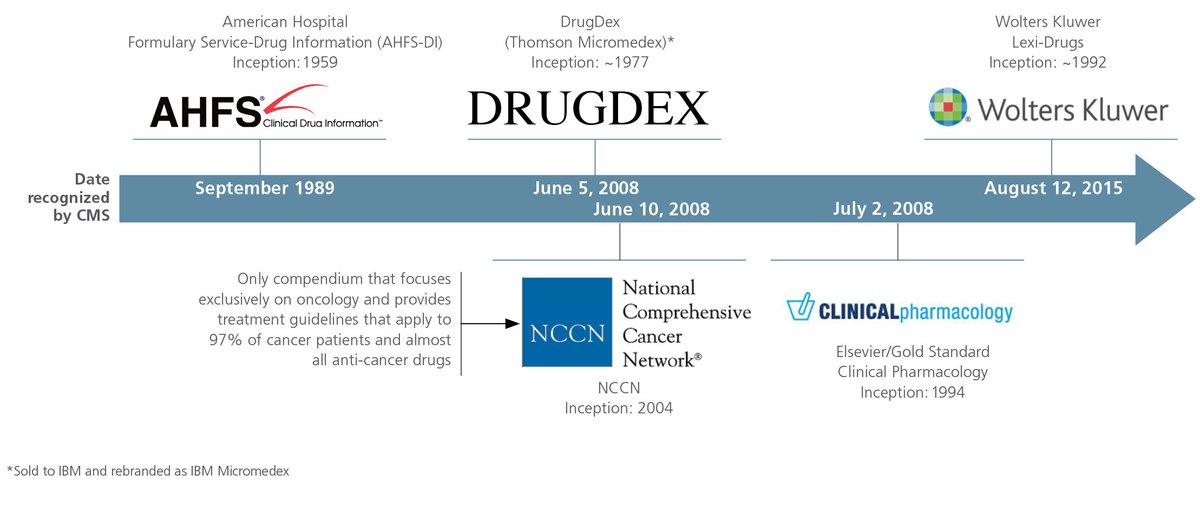
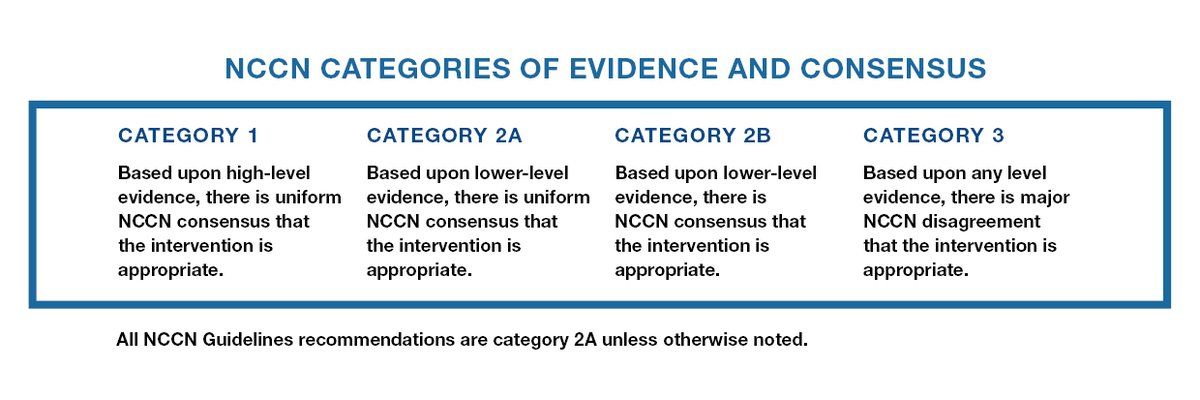
@CMSGov Medicare routinely pays for NCCN "Category 1" and "Category 2A" drugs and some Category 2B; but not usually for Category 3. Private insurers often follow CMS' lead./6
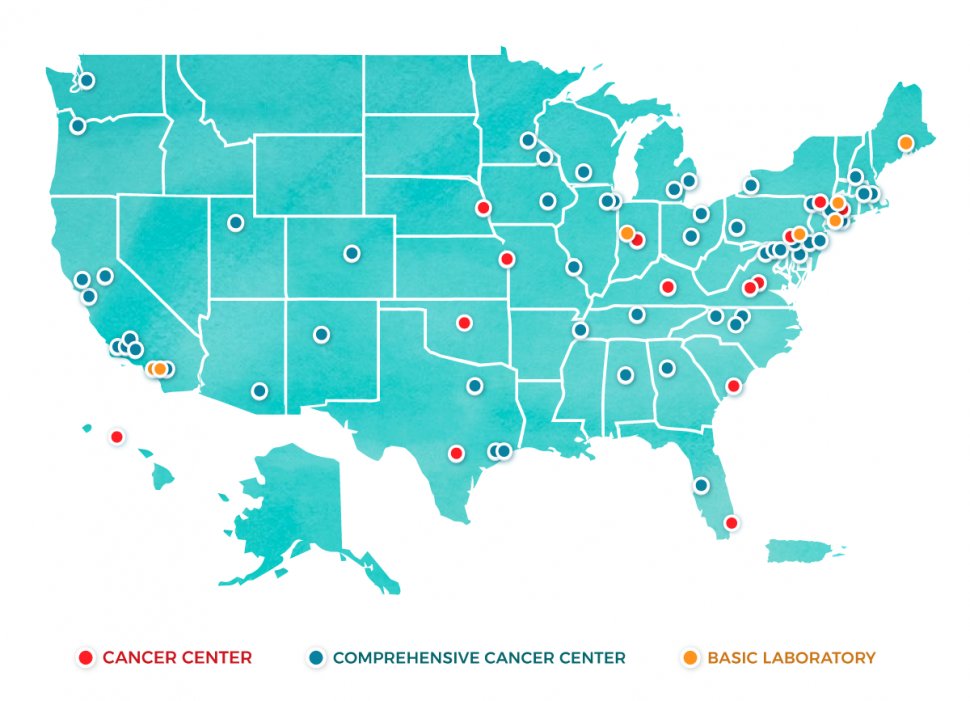
Some history. @NCCN is a private non-profit org that is largely supported by member institutions, of which there are now 30; all are @THeNCI designated cancer centers. There were 13 institutions originally when #NCCN first formed 25 years ago, in 1995./7 nccn.org/members/networ…


Dr. McGivney was succeeded in 2013 by Robert W. Carlson, MD, a breast oncology expert from @StanfordMed. Joining him in 2018 as chief medical officer was Wui-Jin Koh, MD, radiation oncologist at @fredhutch and @SeattleCCA. @NCCN also has a small permanent staff./9

NCCN now has more than 70 different guidelines, reviewed by >1000 panelists, covering: cancer detection, prevention & risk reduction, diagnosis, treatment, and supportive care. These guidelines are said to cover 97% of patients, and are downloaded millions of times each year./10


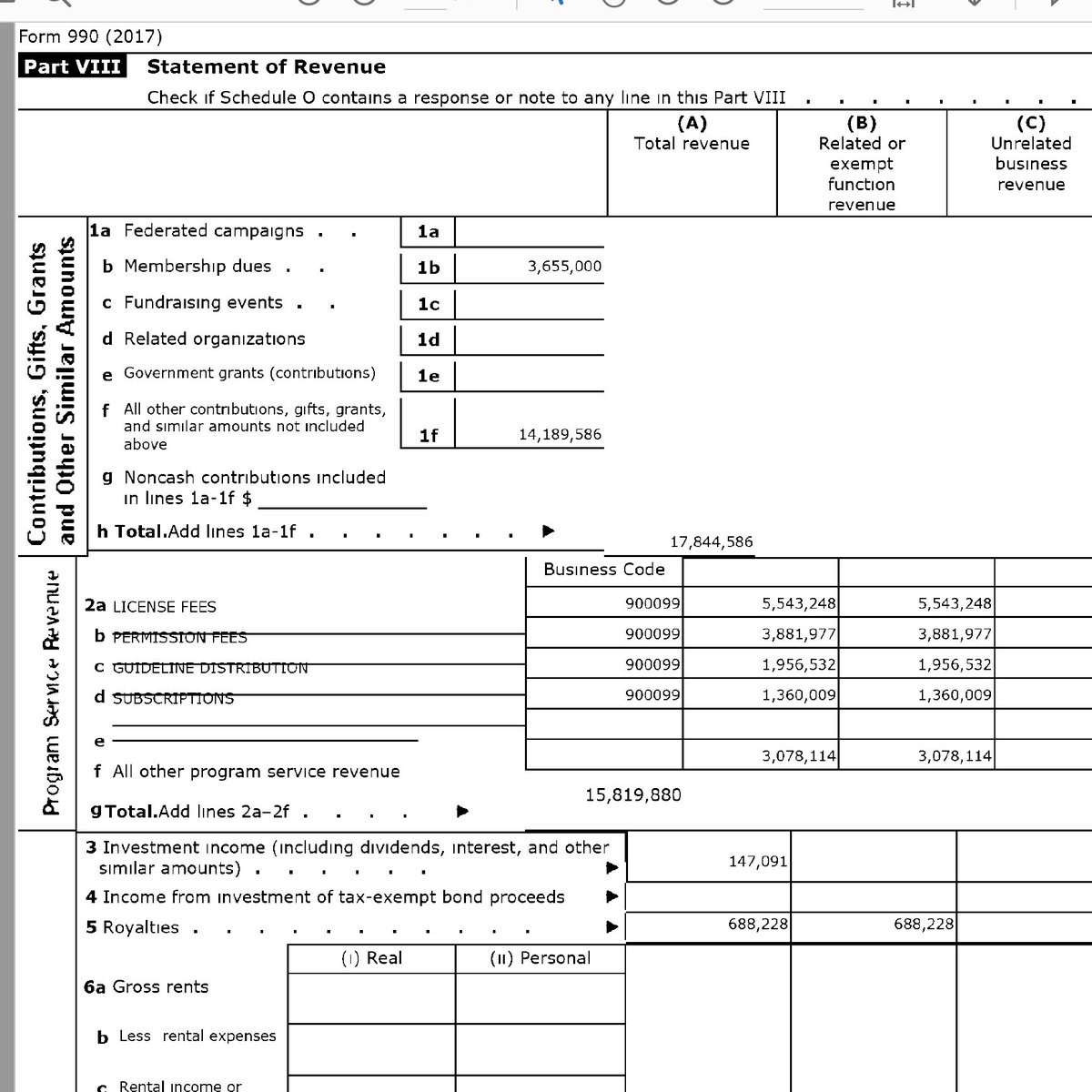
NCCN doesn't include a financial statement in its high quality annual report (or if it does, I can't find it). However, every non-profit organization in the US must file an IRS Form 990, so we can get some information about how @nccn is funded.../11

The latest @NCCN Form 990 that's publicly available is from 2017; it indicates $3.65M total revenue from membership dues. Since there were 27 members in 2017, that suggests median annual dues were ~$135K. Other income comes from grants/contributions ($14M) + $15M license fees./12
@NCCN does other stuff: publishes a journal (@JNCCN) that has a focus on guidelines but includes other oncology-relevant papers; awards Young Investigator & other research grants; and has a Foundation. It also runs a big annual meeting @NCCNMeetings (2020 edition cancelled)./13

First, #FCOI: a 2016 study by @TheWonkologist @dusetzinaS et al found that 84% of guideline panelists had financial conflicts. Since then, I've been told that @NCCN has scrutinized this & asked panel members with more substantive #FCOI to step down./15
jamanetwork.com/journals/jamao…
jamanetwork.com/journals/jamao…
According to @NCCN, “Individuals are disqualified from panel membership if they receive non-research support from industry of >=$20K or more from a single entity or >$50K in aggregate from all entities [per 12 mos]." If no COI were required, it would be hard to find panelists./16

Second, the composition of panels. Some member institutions don’t have a faculty member with deep experience in all 70 guideline areas, yet someone needs to be assigned. At other institutions, there are *multiple* experts in a given area, but there is only 1 seat at the table./17

Should the opinion of someone who "dabbles" part-time in a disease area count the same as someone who has focused their career on that disease for decades? Fairness is important, but that could be interpreted either way. Usually conflicts are amicably resolved, I am told./18

A third controversy is the level of evidence required for a guideline recommendation. In 2018 Wagner et al @VPrasadMDMPH published in @bmj_latest expressing concern that @NCCN justifies coverage of costly, toxic cancer drugs based on weak evidence./19
bmj.com/content/360/bm…
bmj.com/content/360/bm…
A paper by @Dr_R_Kurzrock et al in response defended the @nccn process, and argued that the level of evidence behind guideline recommendations is usually solid and always clearly stated. Guidelines do include long reference lists./20
annalsofoncology.org/article/S0923-…
annalsofoncology.org/article/S0923-…
@Dr_R_Kurzrock concluded, "When the @NCCN recommends beyond the FDA-approved indications, the strength of the evidence supporting such recommendations is robust, with a significant subset of these drugs later becoming @FDAOncology approved or supported by RCT."/21
A fourth critique: the guidelines are permissive, in part due to the important reimbursement implications of inclusion. For some indications, eg B-cell lymphomas, many different regimens are listed as options: a long menu without a lot of guidance on which "entree" to choose./22

This has spurred development of "chef recommendation" tools like @DanaFarber Pathways, spearheaded by my colleague David M. Jackman, to recommend a “best” approach for each scenario based on situation, patient preference, cost considerations, etc./23 dana-farber.org/for-patients-a…
Criticisms aside, @NCCN guidelines are incredibly valuable for practicing clinicians! When I was going out to a satellite clinic & seeing pts with a broader range of conditions than at main site, NCCN guidelines were a helpful reality check on what I was planning to propose.👍/24
For some reason the map with @nccn members didn't show up in the first tweet. Here it is: (Also, for indexing purposes we'll call this thread #HematologyTweetstory 24.)