Here’s my first tweetorial inspired by @OKhaliqueMD. Tips and Tricks on LGE *stealing the title from @VLSorrellImages tinyurl.com/y9yc3ntj
Didn’t know I can tweet on my computer before this. 😀
Didn’t know I can tweet on my computer before this. 😀
For LGE imaging, we generally perform a TI scout, choose TI time to null the myocardium to evaluate for scar (bright). Here blood pool nulls at 145ms, and myocardium nulls at about 240ms 

Alternatively we can use post-contrast T1 map: obtain normal myocardial T1 and multiply by 0.69 or ln(2). E.g. T1: Myo T1 = 422ms, 0.69 * 422 --> normal myocardium nulls at TI of 291ms

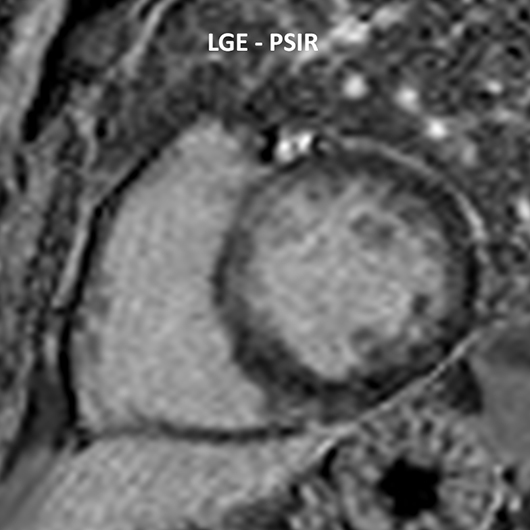
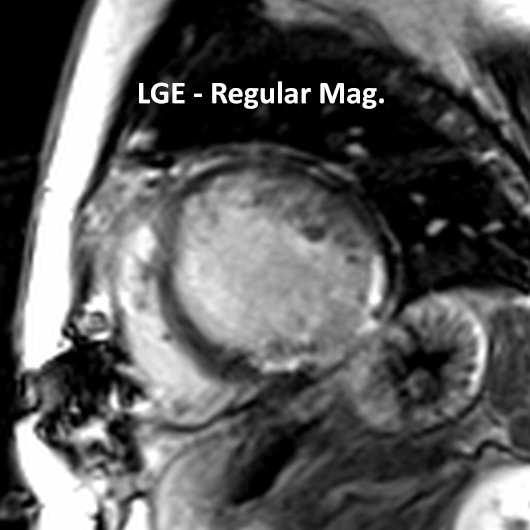
For LGE, we null the myocardium to evaluate for scar (bright). This has inf/inferolateral subendo to transmural scar. Shout out to #SCMR Gold Medal Winners Ray Kim, Bob Judd, @opsimo for dev of LGE tinyurl.com/ya9lprw4 Peter Kellman for PSIR tinyurl.com/yamsdmhg
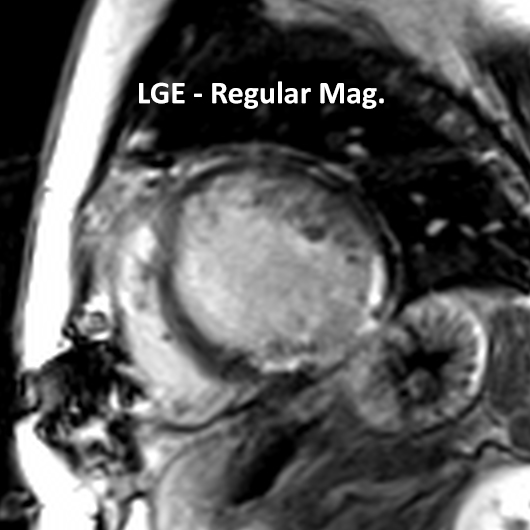
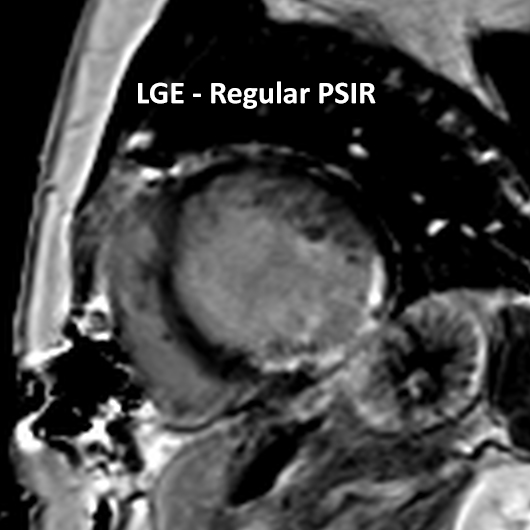
Sometimes, it is difficult to see the enhancement due to the blood is bright as well. There are different techniques to play with to try to improve differentiation of normal myocardium/scar/blood. 0.2mmol/kg can give this CNR problem between scar vs. blood, so use less.
MCODE is a fancy way of doing it, but it’s a research seq developed by #SCMR 2020 Gold Medal Winner Peter Kellman. This acquires a T2 image and an LGE image during the same breath hold so that one can compare blood from myocardium (scar/normal) tinyurl.com/y84eqp3g
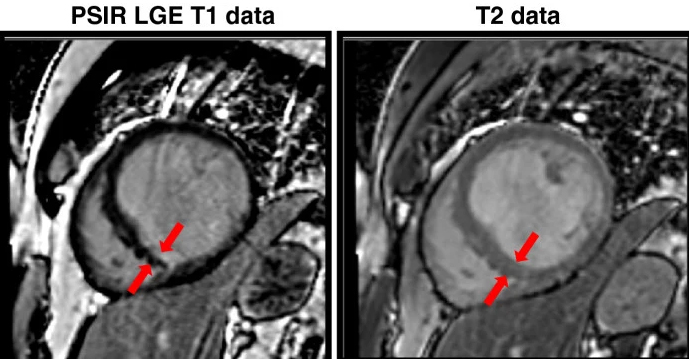
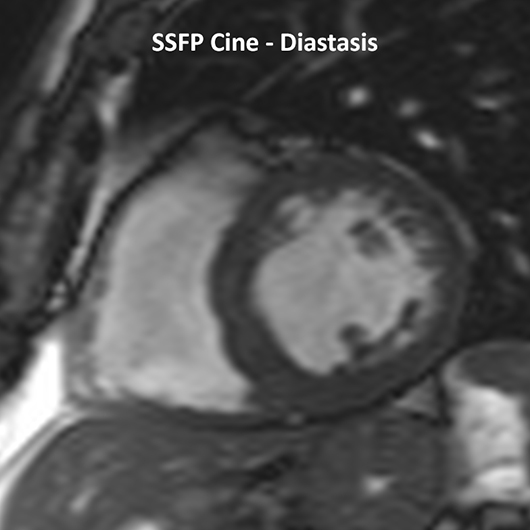
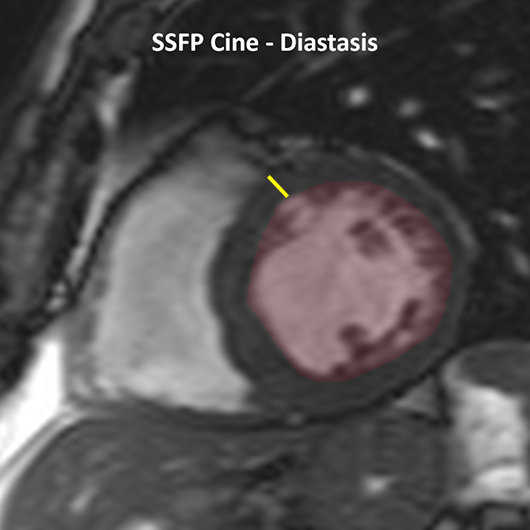
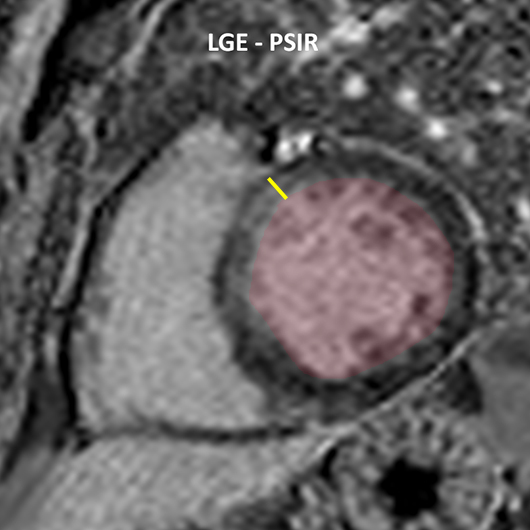
@WPBandettini taught me the “poor man” version of MCODE. We can use SSFP cine image at a similar time in the cardiac cycle, and compare the myocardial thickness to the LGE image to differentiate blood vs. myo enhancement.
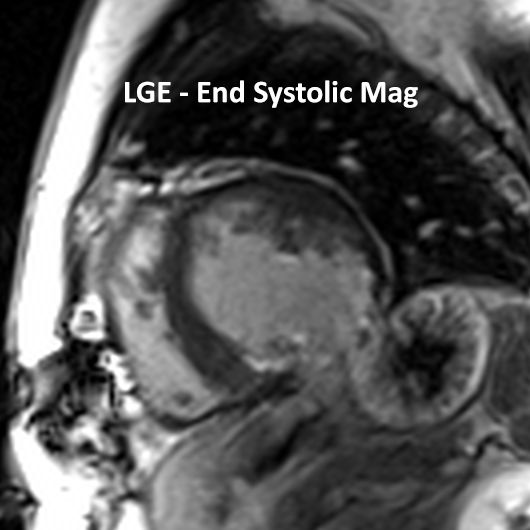
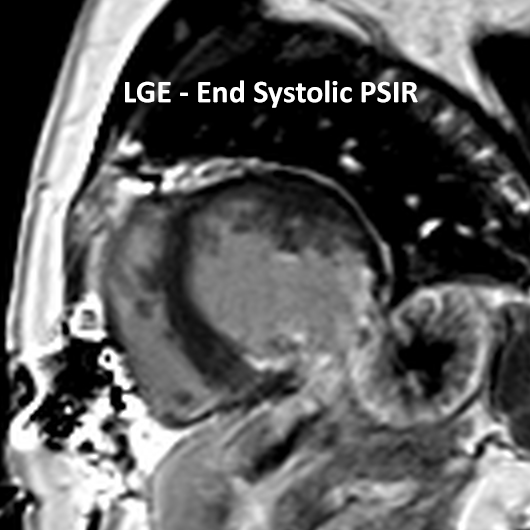
Another method is obtain LGE at end-systole described by 2016 #SCMR Gold Medal Winner @c_eike tinyurl.com/yam2xtje. Normal myo thickens, allow better distinction of scar against nearby myo. Be aware of thru plane motion when compared to diastasis counterpart.

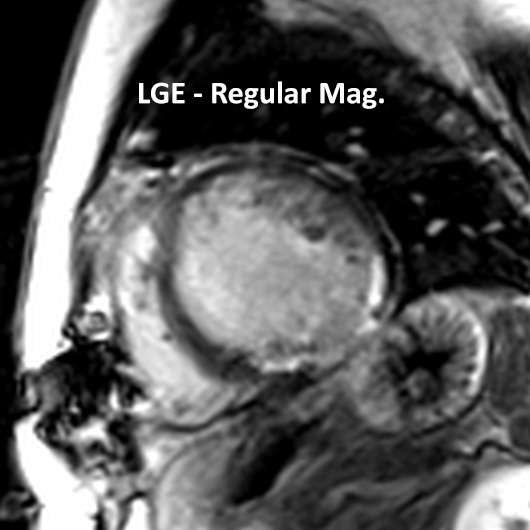
There are various dark blood LGE sequences. One is by 2015 #SCMR Gold Medal Winners Raymond Kim/Bob Judd called FIDDLE tinyurl.com/yckzrtuo. Did you notice the pap muscles on prev images? Another one is tinyurl.com/ydeedgce by Kellman.

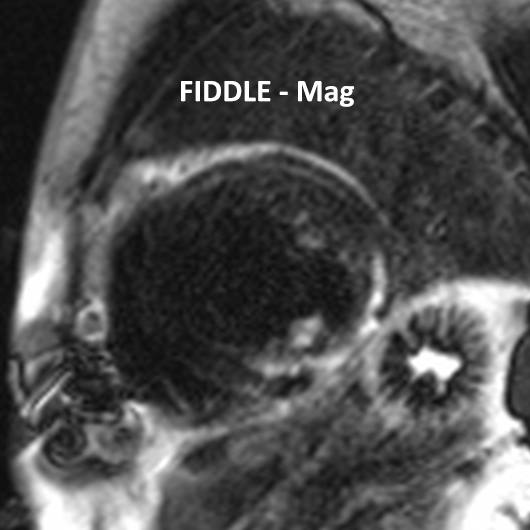
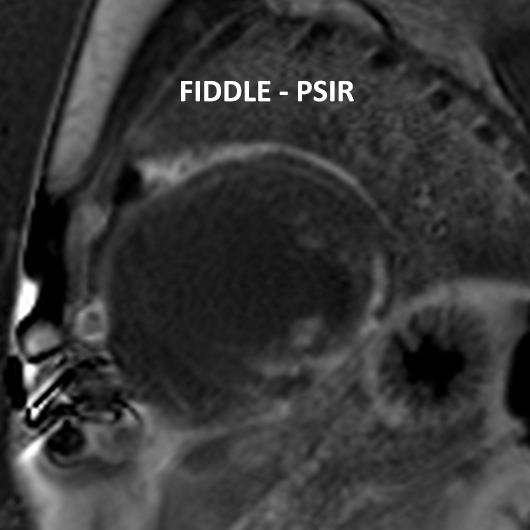
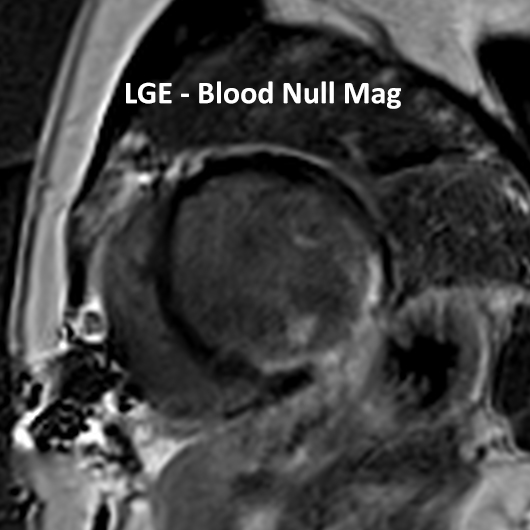
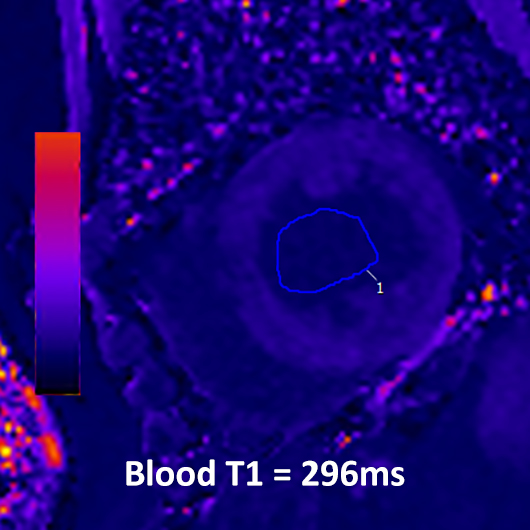
Unfortunately, FIDDLE is a research seq, and so we find workarounds: tinyurl.com/yd2okjsm. We can try to null the blood pool. We would repeat a TI scout or post-contrast T1 map to identify that nulling time. E.g. 0.69 * 296 = 204ms TI time to null blood.
Here’s an example of the same pt with blood nulling LGE (reg LGE seq with TI time set to null the blood). Of note, TI time on this one could have been shorter as normal myo is still darker than the blood. But pap muscles can easily be seen.