
On the eve of world FSHD day (June 20), lets look at Facioscapulohumeral dystrophy / THREAD (1/60) #WorldFSHDDay #FSHD #neuromuscular #dystrophy 
FSHD is one of the MC muscular dystrophies (third MC after DMD and myotonic dystrophy overall and second MC in adults). Still, it’s a rare disease, but if you are seeing neuromuscular patients, you are likely to see FSHD very often pubmed.ncbi.nlm.nih.gov/25122204/
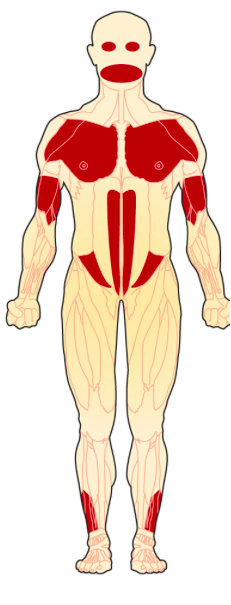
Name is derived from the pattern of muscle involvement➡️ facial, the muscles around the scapula and those overlying humerus. But it also involves trunk and leg muscles. (3/50)
Two genetic subtypes➡️same clinical features:
FSHD1 (95%)- Inherited as Autosomal dominant – 1/3rd Denovo mutations – deletion of large repeat units in Chr4
FSHD2 (5%)- Digenic - requiring mutations in SMCHD1/DNMT3B
Many are asymptomatic carriers (4/60)
FSHD1 (95%)- Inherited as Autosomal dominant – 1/3rd Denovo mutations – deletion of large repeat units in Chr4
FSHD2 (5%)- Digenic - requiring mutations in SMCHD1/DNMT3B
Many are asymptomatic carriers (4/60)

A negative f/h does not rule out FSHD➡️1/3rd of FSHD1 have denovo mutations➡️Asymptomatic carriers in family ➡️Germinal mosaicism (when only parents germ cells are affected- parent appears unaffected but children are at risk) (5/60)

Clinical features: MC presentation is slowly progressive, young adult-onset➡️15-30 years➡️Onset and severity has a wide range➡️Severely affected in infancy to little disability in late 50’s and nonmanifesting carriers. (6/60) pubmed.ncbi.nlm.nih.gov/26862222/
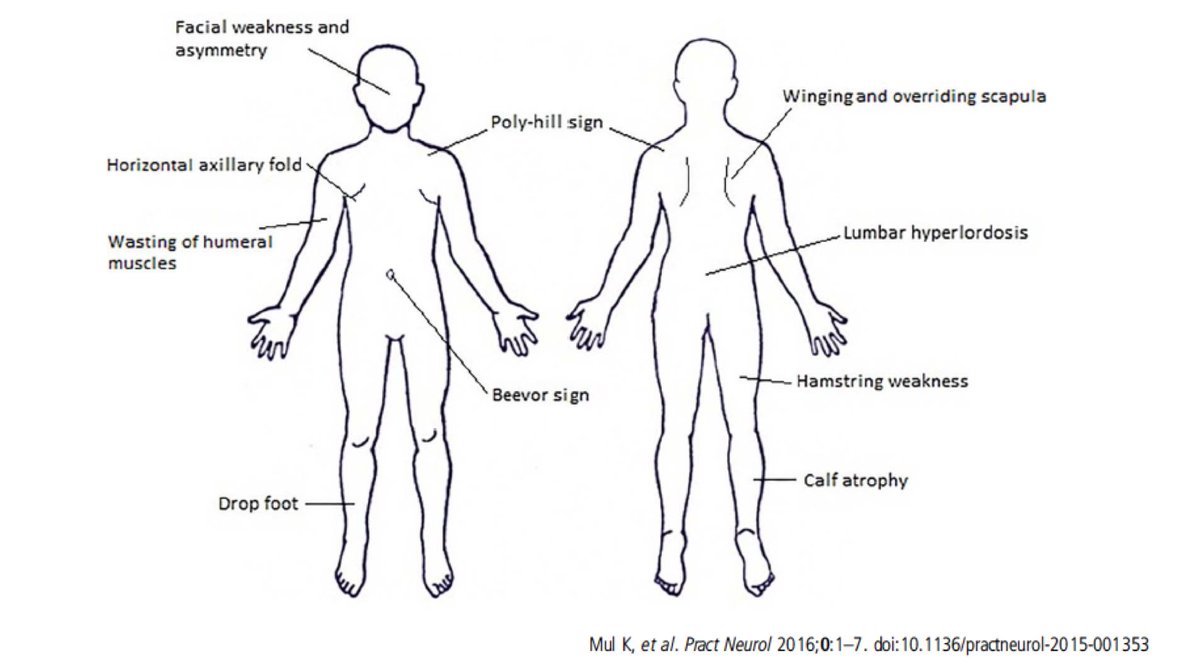
Major symptom: weakness and atrophy in muscles of face and scapula➡️ASYMMETRY is usually very prominent➡️Life expectancy is not affected but it may progress to a disabling disorder➡️Wheel chair dependence in 20% of patients (7/60)
pubmed.ncbi.nlm.nih.gov/31794465/
pubmed.ncbi.nlm.nih.gov/31794465/
Facial muscle weakness is MC➡️but may remain asymptomatic➡️mostly elicited in hindsight🚩But FSHD can present with normal or very minimal facial muscle involvement. (8/60) pubmed.ncbi.nlm.nih.gov/26862222/
Orbicularis oculi weakness➡️Difficulty to close both eyes➡️ Sleeping with eyes partially open▶️Less pronounced weakness can lead to ‘signe de cils’⏺️inability to bury the eyelashes completely while closing eyes tightly (9/60)
pubmed.ncbi.nlm.nih.gov/26862222/
pubmed.ncbi.nlm.nih.gov/26862222/
Zygomaticus muscle weakness➡️inability to raise the corners of the mouth▶️On attempting to smile, the mouth moves horizontally➡️ ‘transverse smile’➡️could very well be an ‘asymmetric’ smile (10/60) pubmed.ncbi.nlm.nih.gov/26862222/
Infants with facial weakness➡️Inability to suck▶️no social smile➡️More severe disease (11/60)
Finally, once all facial muscles are involved▶️unwrinkled and expressionless ‘myopathic face’ 🚩Extra-ocular muscles (EOM) are NEVER affected (12/60)
Weakness of muscles of scapular fixation▶️Trapezius and Serratus Anterior▶️leads to winging of scapula▶️bilateral and asymmetrical ⏺️Overriding scapula▶️an upward movement of the scapula due to loss of its inferior fixation (13/60) pubmed.ncbi.nlm.nih.gov/25772187/
Polyhill sign▶️Due to selective wasting of muscles1⃣atrophy of trapezius + upward movement of superior angle of scapula2⃣displaced acromioclavicular joint3⃣Preserved distal deltoid4⃣Bulge due to brachioradialis or EDC(14/60) pubmed.ncbi.nlm.nih.gov/11994973/

Sometimes there can be ‘Extra’ hills too▶️bulge in middle of biceps▶️But once can see variations in hills in many cases (15/60) pubmed.ncbi.nlm.nih.gov/18040140/
CF▶️Inability to abduct arms to 180 degree but may throw their arms up▶️Pectoralis weakness leads to horizontal clavicle and deep axillary creases (15/50) pubmed.ncbi.nlm.nih.gov/26862222/
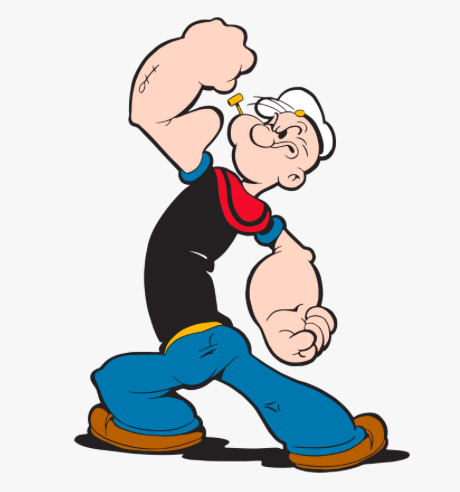
Popeye arm▶️Biceps and triceps more involved than distal deltoid and forearm muscles (17/60) pubmed.ncbi.nlm.nih.gov/26862222/
neurosigns.org/wiki/Popeye_arm
neurosigns.org/wiki/Popeye_arm
Lordosis and protuberant abdomen▶️paraspinal and abdominal muscle weakness (18/60)

Bevor sign▶️upward movement of the umbilicus on flexing the neck in the supine position➡️Because of the differential weakness of lower part of the rectus abdominis
the umbilicus gets pulled upwards(19/60)
pubmed.ncbi.nlm.nih.gov/19838767/
the umbilicus gets pulled upwards(19/60)
pubmed.ncbi.nlm.nih.gov/19838767/
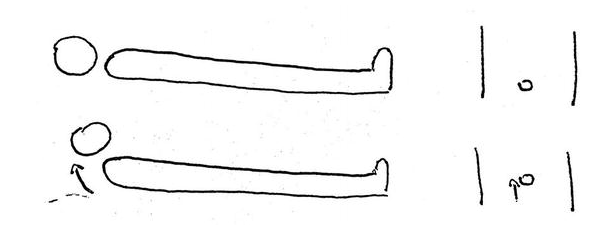
Erector spinae muscle weakness▶️‘bent spine syndrome’ or camptocormia (20/60) pubmed.ncbi.nlm.nih.gov/25156185/
Combined weakness of abdominal and back muscles▶️loss of balance and frequent falls (21/60) pubmed.ncbi.nlm.nih.gov/25156185/
Unilateral pelvic tilt▶️asymmetric hip muscle involvement (22/60) pubmed.ncbi.nlm.nih.gov/26862222/
⏺️Foot drop due to TA weakness ⏺️EDB hypertrophy
pubmed.ncbi.nlm.nih.gov/22079131/
pubmed.ncbi.nlm.nih.gov/605779/
pubmed.ncbi.nlm.nih.gov/22079131/
pubmed.ncbi.nlm.nih.gov/605779/
Clinical clues:
⏺️Neck extensors more affected than flexors
⏺️Biceps>Triceps
⏺️Contractures are absent or minimal
⏺️No significant cardiac involvement
⏺️Preserved distal deltoid, supraspinatus and infraspinatus muscles (24/60) pubmed.ncbi.nlm.nih.gov/29478599/
⏺️Neck extensors more affected than flexors
⏺️Biceps>Triceps
⏺️Contractures are absent or minimal
⏺️No significant cardiac involvement
⏺️Preserved distal deltoid, supraspinatus and infraspinatus muscles (24/60) pubmed.ncbi.nlm.nih.gov/29478599/
In contrast to other dystrophies, FSHD develops atrophy earlier and does not frequently go through a phase of hypertrophy (25/60)
Isolated presentations which may be overlooked:
⏺️Isolated unilateral foot drop
⏺️Shoulder complaints
⏺️Frequent falls
⏺️Pectus excavatum
⏺️Back pain and fatigue (26/60)
pubmed.ncbi.nlm.nih.gov/26862222/
⏺️Isolated unilateral foot drop
⏺️Shoulder complaints
⏺️Frequent falls
⏺️Pectus excavatum
⏺️Back pain and fatigue (26/60)
pubmed.ncbi.nlm.nih.gov/26862222/
Associated symptoms in FSHD:
⏺️Resp failure requiring ventilatory support is rare
⏺️But 1/3rd of nonambulatory FSHD have Resp involvement
⏺️Nocturnal hypoventilation
⏺️No significant cardiac involvement (27/60)
⏺️Resp failure requiring ventilatory support is rare
⏺️But 1/3rd of nonambulatory FSHD have Resp involvement
⏺️Nocturnal hypoventilation
⏺️No significant cardiac involvement (27/60)
Associated symptoms in FSHD:
⏺️FSHD1 – Retinal vasculopathy- telegiectasias, microaneurysms, Coats disease
⏺️Severe retinal vasculopathy, Hearing loss▶️ large 4q35 deletions
⏺️Musculoskeletal pain is very frequent (28/60)
pubmed.ncbi.nlm.nih.gov/29478599/
⏺️FSHD1 – Retinal vasculopathy- telegiectasias, microaneurysms, Coats disease
⏺️Severe retinal vasculopathy, Hearing loss▶️ large 4q35 deletions
⏺️Musculoskeletal pain is very frequent (28/60)
pubmed.ncbi.nlm.nih.gov/29478599/
🚩Red flags
🚫Ptosis
🚫EOM involvement
🚫Bulbar involvement
🚫Contractures
🚫Cardiomyopathy
🚫Significant resp involvement in mild weakness (29/60)
pubmed.ncbi.nlm.nih.gov/29478599/
🚫Ptosis
🚫EOM involvement
🚫Bulbar involvement
🚫Contractures
🚫Cardiomyopathy
🚫Significant resp involvement in mild weakness (29/60)
pubmed.ncbi.nlm.nih.gov/29478599/
Investigations
▶️Creatine Kinase: Normal to mildly elevated
▶️EMG: Myopathic – may show evidence of irritability (PSW and Fibs) (30/60)
▶️Creatine Kinase: Normal to mildly elevated
▶️EMG: Myopathic – may show evidence of irritability (PSW and Fibs) (30/60)
Muscle MRI
▶️Mostly done in research setting
▶️Great potential to be a clinical trial outcome measure ▶️Rectus abdominis and semimembranosus are the MC and most severely affected muscles (31/60)
pubmed.ncbi.nlm.nih.gov/25641525/
▶️Mostly done in research setting
▶️Great potential to be a clinical trial outcome measure ▶️Rectus abdominis and semimembranosus are the MC and most severely affected muscles (31/60)
pubmed.ncbi.nlm.nih.gov/25641525/
Biopsy▶️Nonspecific myopathic features with 1/3rd cases showing endomysial inflammation (32/60)
Genetics of FSHD: Ok, if u have reached till here- u r really patient. Now I am going out of my comfort zone. If I get any of these complex facts wrong, pls correct me 🙏 (33/60)
Genetics: FSHD is a toxic gain-of-function disease, where a gene contained in the D4Z4 repeats on chromosome 4 (which is normally silent), DUX4, gets “turned on”. (34/60) pubmed.ncbi.nlm.nih.gov/14634647/
Genetics: Normally distal end of both copies of Chromosome 4q35 contain microsatellite repeat arrays which consists of 11–100 D4Z4 repeats which is methylated adequately as in a transcriptionally silent heterochromatic region (35/60) pubmed.ncbi.nlm.nih.gov/31979100/
D4Z4 repeats contain 2 exons and open reading frame for DUX4 gene (36/60) pubmed.ncbi.nlm.nih.gov/10433963/
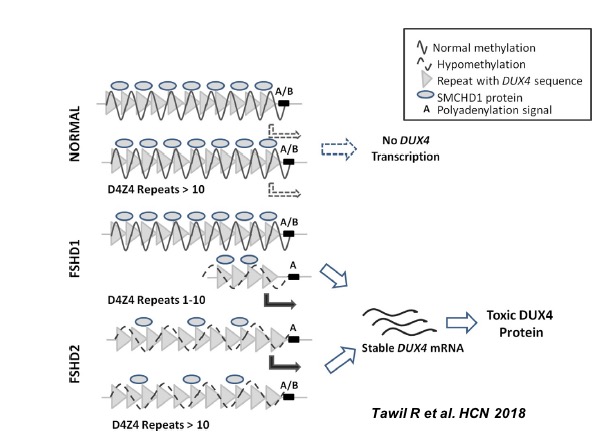
In FSHD1, there is contraction of repeats (1-10) in one copy of 4q35 and associated hypomethylation which leads to relaxation of chromatin and DUX4 gene is transcribed.(37/60) ncbi.nlm.nih.gov/books/NBK1443/
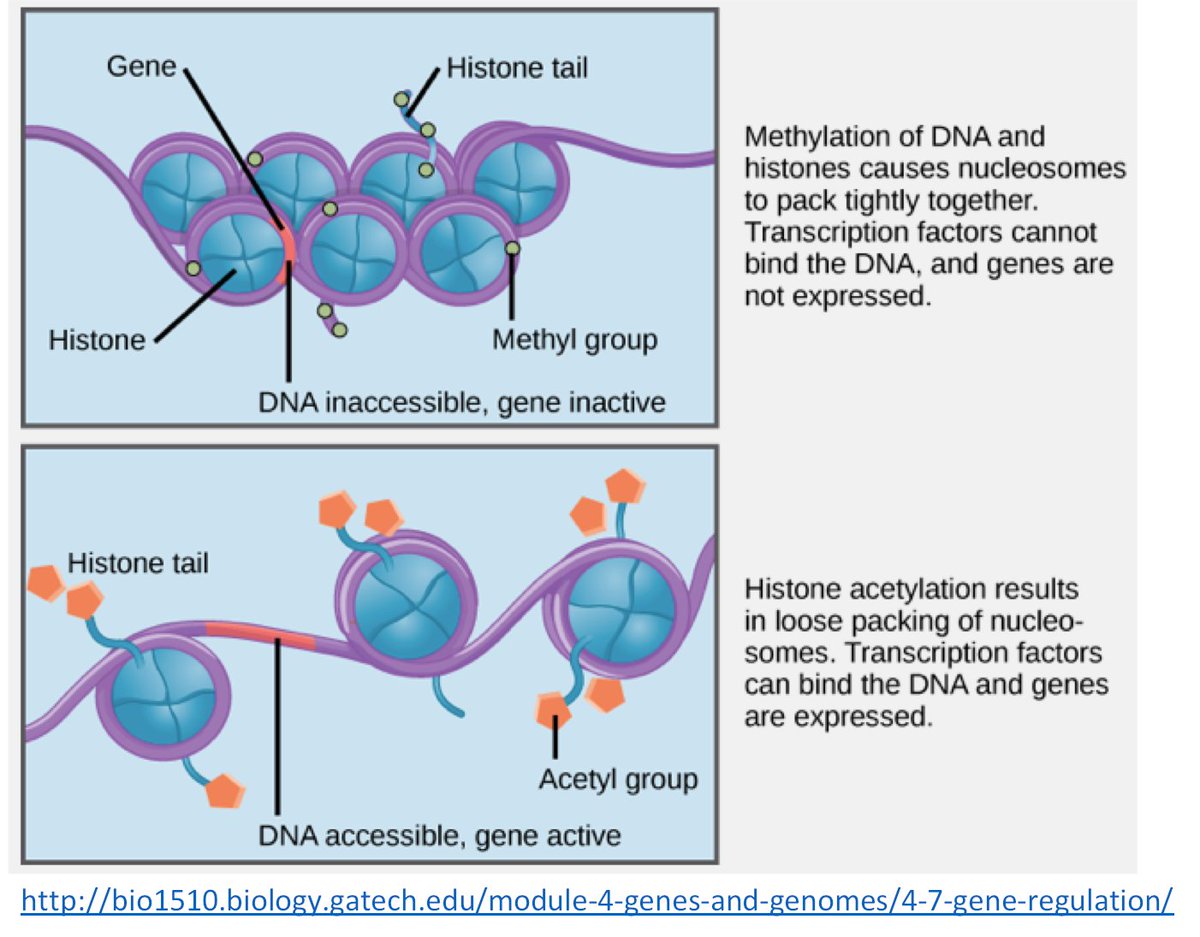
In FSHD2, both copies of 4q35 may have normal repeats but the DNA is hypomethylated due to mutations in either SMCHD1 gene on Chr 18 or DNMT3B gene resulting in a more permissive chromatin structure (38/60) pubmed.ncbi.nlm.nih.gov/31794465/
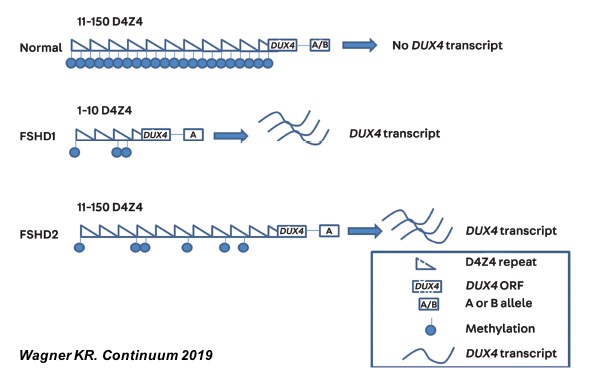
⏺️Either repeat contraction (FSHD1) or hypomethylation (FSHD2) is necessary but not sufficient enough
⏺️Stable DUX4 mRNA can happen only if there is a polyadenylation sequence distal to the last repeat (A-allele) (39/60) pubmed.ncbi.nlm.nih.gov/29478599/
⏺️Stable DUX4 mRNA can happen only if there is a polyadenylation sequence distal to the last repeat (A-allele) (39/60) pubmed.ncbi.nlm.nih.gov/29478599/
Atleast one D4Z4 repeats should be there▶️ if the whole D4Z4 is deleted▶️no FSHD (40/60)
Unifying model▶️In a permissive 4qA haplotype, hypomethylation of D4Z4 region of Chr.4q35 (contraction of D4Z4 or SMCHD1/DNMT3B mutation) results in opening of chromatin structure and production of stable DUX4 mRNA/protein (41/60) pubmed.ncbi.nlm.nih.gov/20724583/
In other words, with a 4qA haplotype, these mutations cause loss of epigenetic silencing of the D4Z4 array resulting in DUX4 transcription (42/60)
Keywords in FSHD Genetics
⏺️D4Z4 repeat contraction
⏺️hypomethylation
⏺️chromatin relaxation
⏺️poly-A tail (A-allele)
⏺️DUX4 transcription
⏺️epigenetic de-repression (43/60)
⏺️D4Z4 repeat contraction
⏺️hypomethylation
⏺️chromatin relaxation
⏺️poly-A tail (A-allele)
⏺️DUX4 transcription
⏺️epigenetic de-repression (43/60)
Asymptomatic carriers carry a permissive Chromosome 4 but lack the ‘adequate’ D4Z4 hypomethylation (44/60) pubmed.ncbi.nlm.nih.gov/25031281/

Pathophysiology▶️ DUX4 is the bad guy
⏺️Aberrant expression of DUX4 protein in somatic cells is the primary cause
⏺️DUX4 is normally expressed in germline but repressed in somatic tissue. pubmed.ncbi.nlm.nih.gov/15674778/
⏺️Aberrant expression of DUX4 protein in somatic cells is the primary cause
⏺️DUX4 is normally expressed in germline but repressed in somatic tissue. pubmed.ncbi.nlm.nih.gov/15674778/
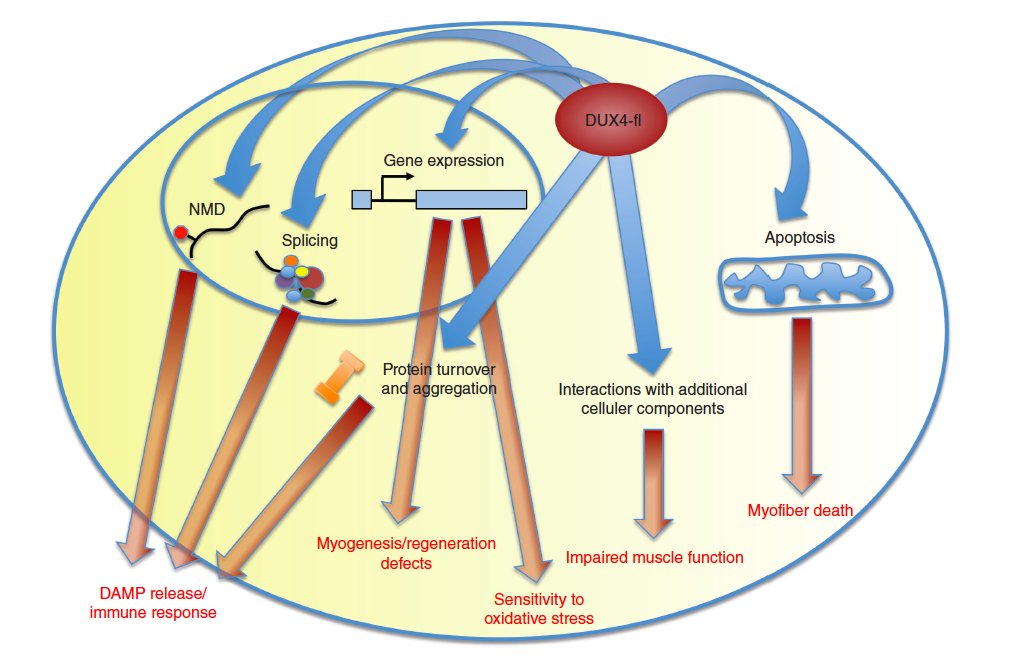
⏺️DUX4 protein is highly toxic and causes apoptosis
⏺️DUX4 also activates various genes involved in atrophy, protein degradation, oxidative stress, and innate immunity. (46/60) pubmed.ncbi.nlm.nih.gov/28915324/
⏺️DUX4 also activates various genes involved in atrophy, protein degradation, oxidative stress, and innate immunity. (46/60) pubmed.ncbi.nlm.nih.gov/28915324/
Inflammation in FSHD
▶️Proteins expressed only in the germline may induce an immune response when aberrantly expressed in somatic tissue, as germline is immune-privileged (47/60) pubmed.ncbi.nlm.nih.gov/29478599/
▶️Proteins expressed only in the germline may induce an immune response when aberrantly expressed in somatic tissue, as germline is immune-privileged (47/60) pubmed.ncbi.nlm.nih.gov/29478599/
But how a rare event like DUX4 transcription in only a few nuclei can trigger worsening of entire muscle fibers? Ans: Nuclear protein spreading (48/60) pubmed.ncbi.nlm.nih.gov/29478599/
DUX4 transcription occurs in very few nuclei▶️protein formed diffuses into nearby nuclei within the myotubes▶️creates a gradient▶️spreading aberrant gene expression (49/60) pubmed.ncbi.nlm.nih.gov/24659496/
Nuclear protein spreading mechanism may explain a common clinical phenomenon in FSHD:
⏺️Muscles may look very normal initially▶️then one muscle gets affected▶️very quickly another one gets involved as if ‘disease is travelling along the muscle’ (50/60)
⏺️Muscles may look very normal initially▶️then one muscle gets affected▶️very quickly another one gets involved as if ‘disease is travelling along the muscle’ (50/60)
Now this also leads to a controversial hypothesis that severe exercise may kick off this nuclear protein spread but its NOT yet proven! (51/60)
How does one get about with genetic testing in an individual patient ? At present, Exome sequencing techniques cannot detect FSHD1 (52/60)
So first look for contraction of the 4q35 subtelomeric region (pulsed field electrophoresis + Southern blotting) followed by haplotype testing. (53/60) pubmed.ncbi.nlm.nih.gov/26215877/
⏺️If Haplotype is A and restricted fragment is 10kb to 28kb (normal > 38 kb) which corresponds to 1-10 D4Z4 repeats▶️FSHD1 can be confirmed
⏺️If methylation is very low (<20%) in haplotype A▶️FSHD2- look for mutation in SMCHD1 (54/60)
⏺️If methylation is very low (<20%) in haplotype A▶️FSHD2- look for mutation in SMCHD1 (54/60)

Prognosis based on genetic diagnosis (55/60)

No disease modifying treatment available. Various therapeutic approaches are targeting DUX4 (56/60)

⏺️All FSHD patients should undergo vision and hearing assessment especially those with large 4q
⏺️Pulmonary function testing should be done at baseline especially those with severe proximal weakness, kyphoscoliosis, or wheelchair dependence(57/60)
⏺️Pulmonary function testing should be done at baseline especially those with severe proximal weakness, kyphoscoliosis, or wheelchair dependence(57/60)
⏺️Management of pain: physical therapy, NSAIDS, ⏺️Duloxetine Ankle-foot orthosis for foot drop.
⏺️Low intensity aerobic exercise
⏺️Bone health – Vitamin D3 if needed. DXA scans annually in those with severe weakness, falls or wheel chair dependent (58/60)
⏺️Low intensity aerobic exercise
⏺️Bone health – Vitamin D3 if needed. DXA scans annually in those with severe weakness, falls or wheel chair dependent (58/60)
Surgical scapular fixation to rib
▶️Patient should have good deltoid power to get benefit. ▶️It’s an extensive procedure and should be done only by an experienced surgeon
▶️Patient may not be able to throw the arm up to 180 degree as before (59/60)
▶️Patient should have good deltoid power to get benefit. ▶️It’s an extensive procedure and should be done only by an experienced surgeon
▶️Patient may not be able to throw the arm up to 180 degree as before (59/60)
Conclusion: Lot of exciting developments in FSHD research especially genetics which has the potential to bring disease modifying therapies in near future. Many thanks to Prof.Thomas Voit who gave @ICGNMD fellows a glimpse to genetics of FSHD.

