Thoughts on RECOVERY preprint: dexamethasone as treatment for COVID-19 @AaronRichterman medrxiv.org/content/10.110…


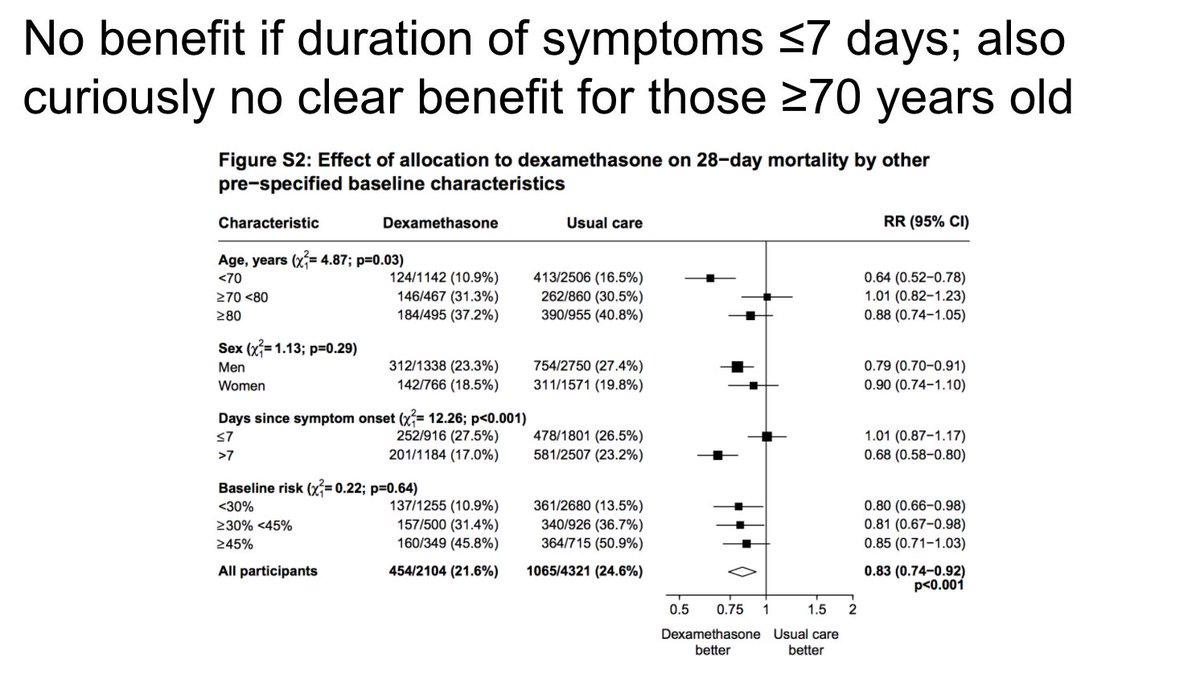
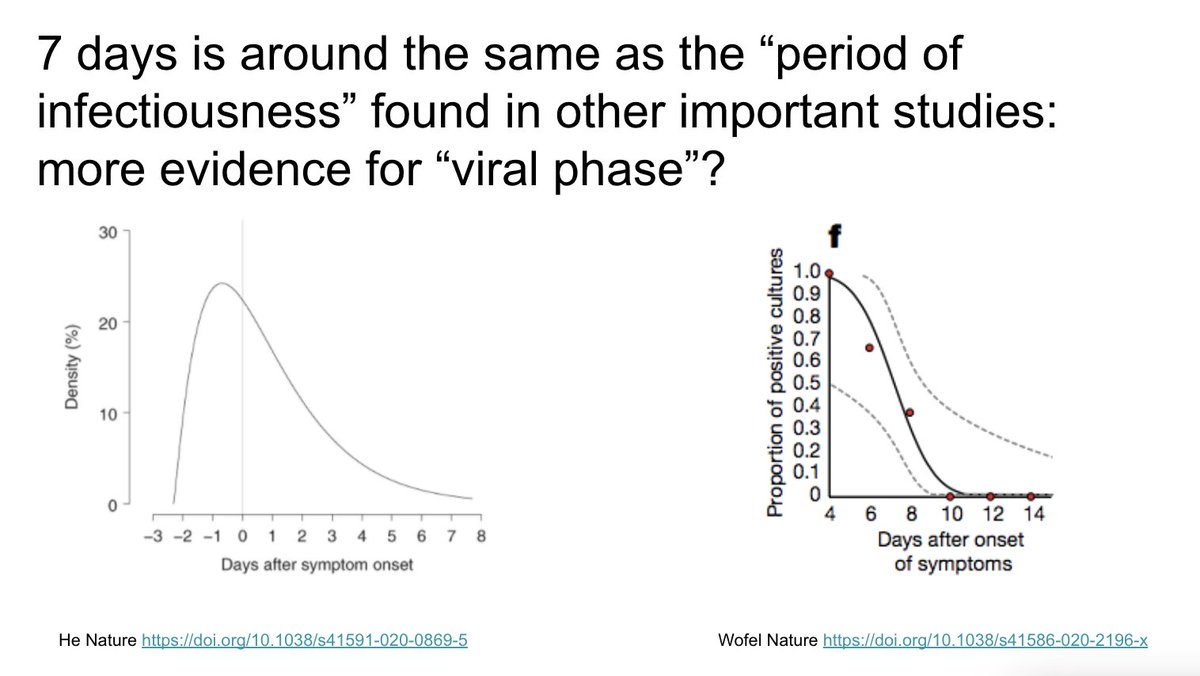
Is the finding of no benefit before 7 days of symptoms possibly more evidence for a "viral phase"? There has been a theoretical concern that steroids given during "viral phase" could increase period of viral shedding/replication 
Given known heterogeneity in COVID-19 presentations, data on CRP, ferritin, D-dimer, and other lab markers could potentially help providers identity those individuals more likely to benefit from steroids by defining parameters for hyperinflammatory pneumonia
After talking with some brilliant colleagues, I have some additions for this thread. Thanks to so many in @mgh_id for constant conversation and discussion about this
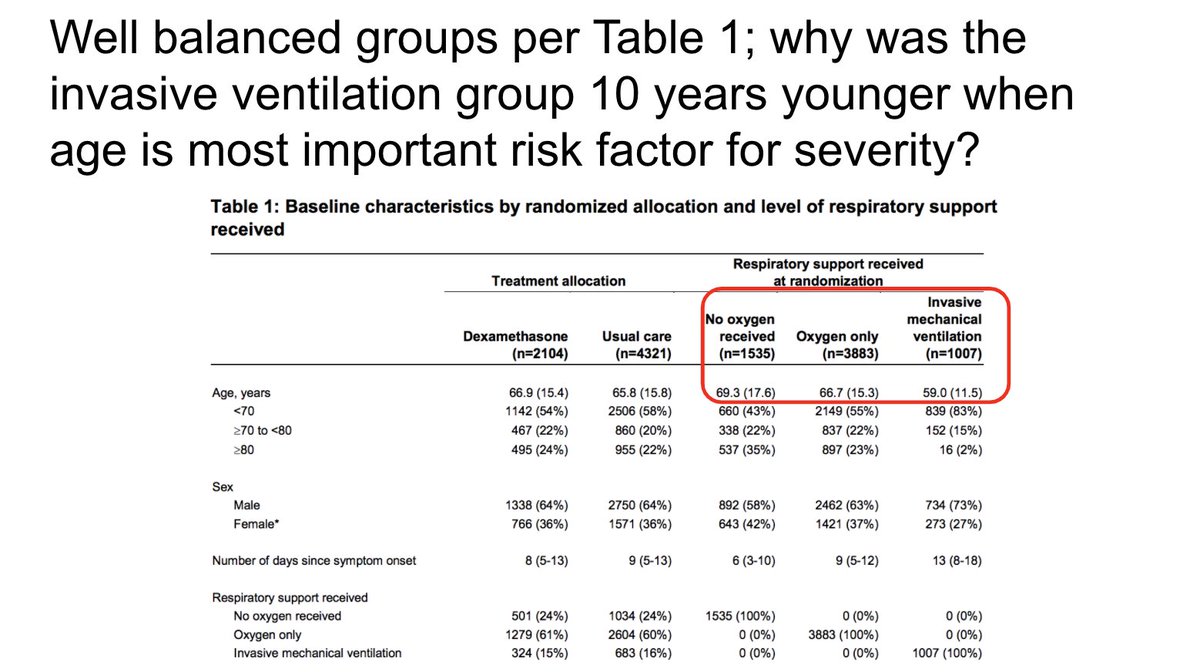
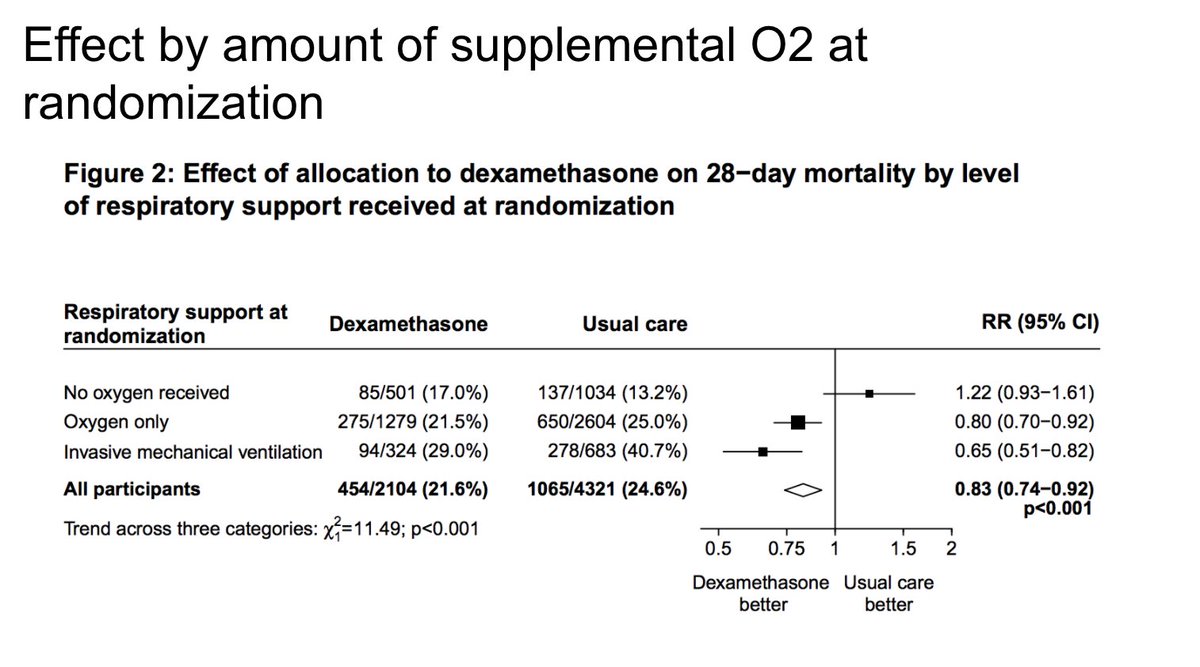
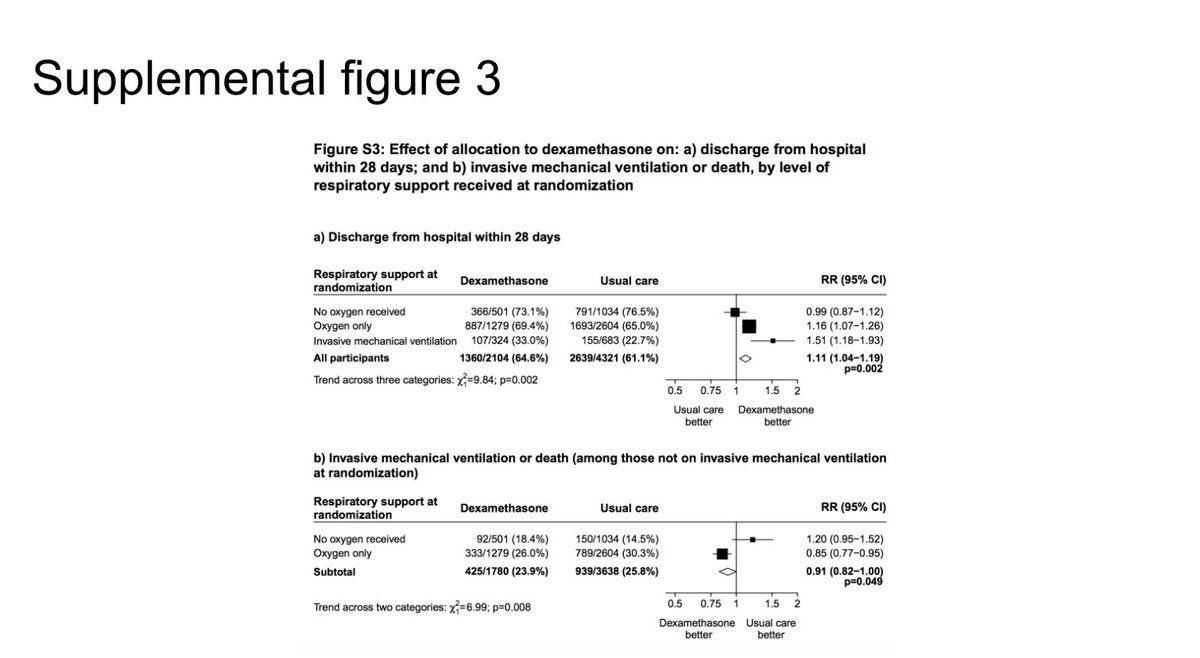
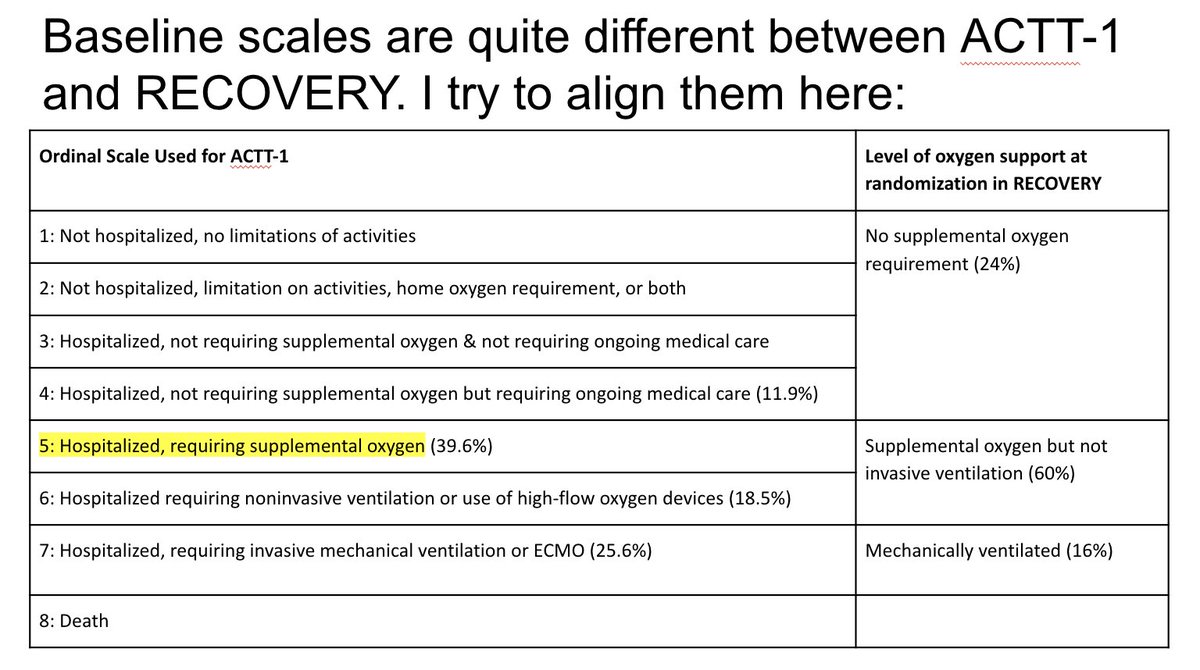
It's key to remember the differences between the baseline statuses of RECOVERY/ACTT-1. "Supplemental oxygen" category in RECOVERY is broad and includes baseline ordinal level 5 & 6 in ACTT-1
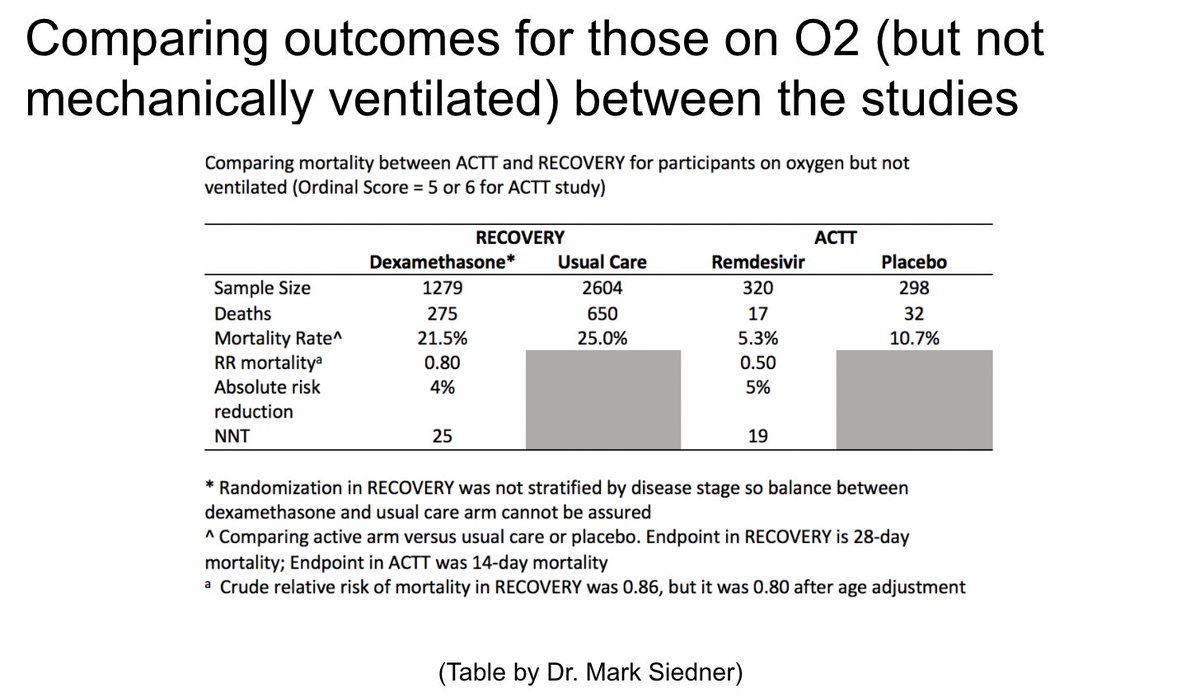
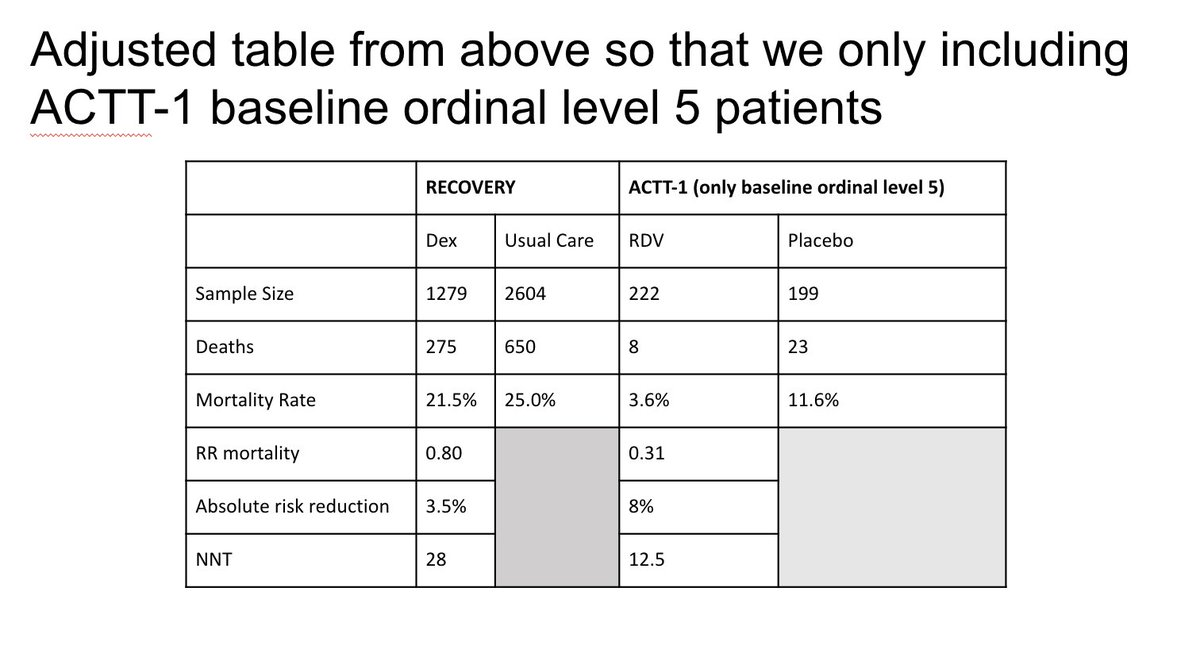
Dr. Mark Siedner (not on twitter??) made this table and gave me permission to share. Note many more people in RECOVERY. Also note the "usual care" of RECOVERY has >2x mortality of ACTT-1. Importantly as Mark points out: 14-day mortality for ACTT-1 vs 28-day for RECOVERY
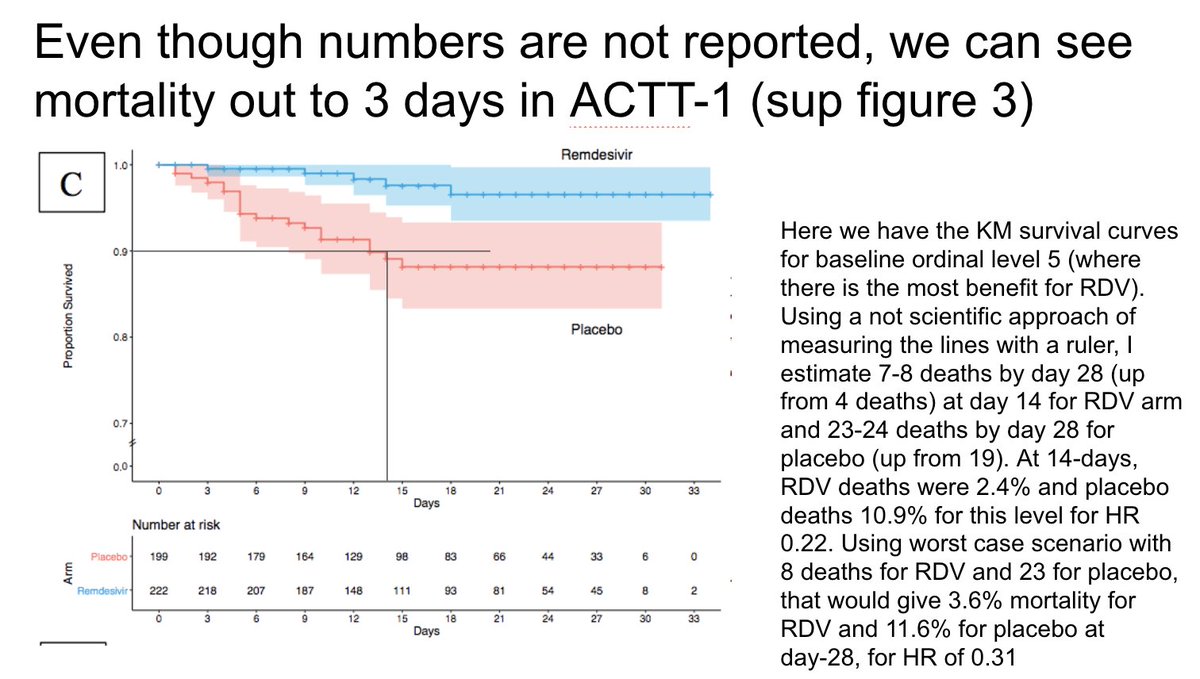
Though we 28-day mortality data is not directly reported from ACTT-1, the supplementary figure 3 includes this KM curve that extends past 30 days. Note at 30-days there are <10 people in each group without full data. I tried to calculate mortality at 28 days from this figure
Here is an adjusted table exactly like Mark's above except that for the ACTT-1 data I'm only using baseline ordinal level 5 where we know the highest benefit is
My conclusion (very open to other opinions) is that there is more extensive data available from ACTT-1 that allows for better differentiation between subgroups and therefore selection of people very likely to benefit (ie baseline ordinal level 5, very low NNT)
On the other hand, while there is clearly a subgroup that benefits from dexamethasone (including outside of ICU), I think we need more data to be able to deploy this medication most effective.
I stand by what I wrote last night. For a patient with baseline ordinal level 5 as in the ACTT-1 trial, I would recommend RDV and likely not dex initially. (Though if they progressed I would absolutely start dex)