Let’s talk about the really good news out last week about dexamethasone (“dex” as we docs lovingly call it) to treat serious COVID19. And let’s also talk about rapid scientific announcements, flatting the curve, and the declining COVID19 fatality rate seen these days. 1/
This is indeed a meaningful advance. Dex – a widely available, cheap, and well understood drug – reduces (but doesn’t eliminate) mortality from serious COVID19. Publicly announced on June 18, 2020 and posted on @medrxivpreprint on June 22. medrxiv.org/content/10.110… 2/
Roughly speaking, the investigators report preventing one death for every 10 patients who get to the ventilator stage. Since about 4 of those 10 patients would have died, dex prevents nearly 1 out of 4 deaths of very sick patients. 3/
Hence, to be clear, most deaths from COVID19 will still occur. We do not yet have any way to prevent or cure COVID-19. But this RCT is still very good news. 4/
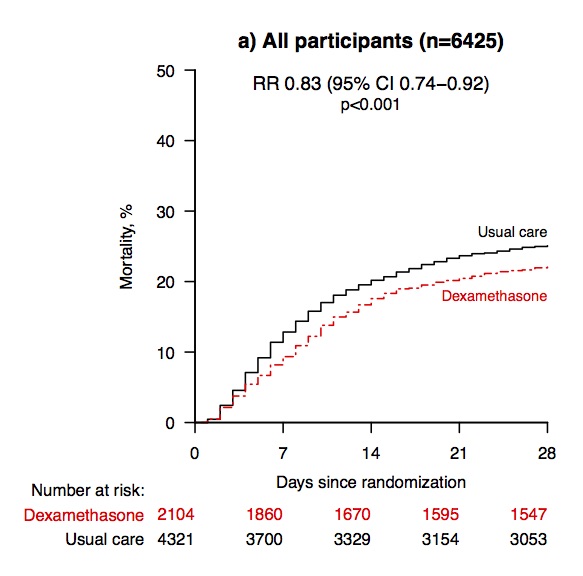
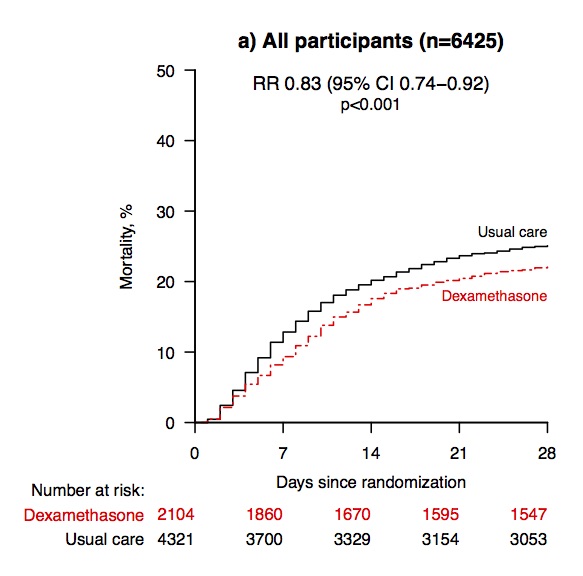
In this landmark RCT, 2,104 hospitalized COVID19 patients were randomized to receive dexamethasone ("dex") 6 mg daily (oral/IV) for 10 days, and 4,321 patients got usual care (though 7% of these patients also got dex at their own doc's orders). They were followed for 28 days. 5/
Mean patient age was ~66 years old and 64% of patients were men. They were hospitalized with COVID19 in the UK, getting excellent care. But still, COVID19 is a serious disease: overall, 23.6% of the patients in the trial died by 28 days. 6/
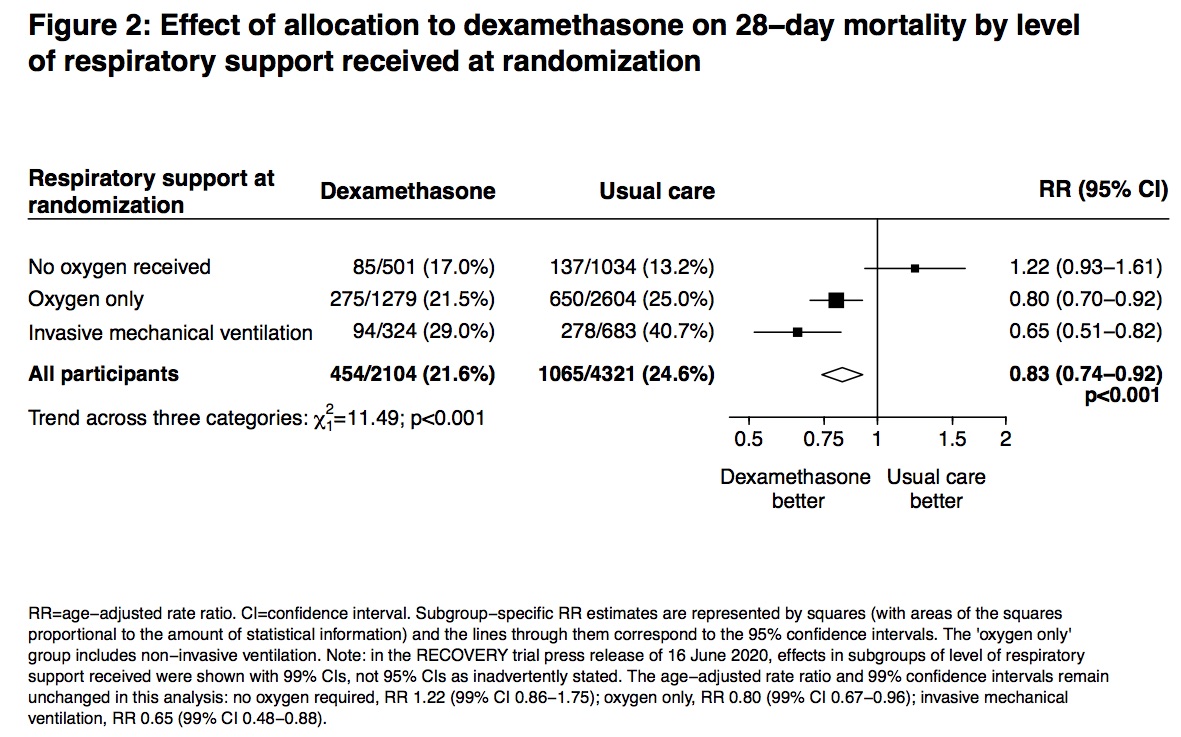
Overall, 21.6% of the dex patients died and 24.6% of the usual care patients died. Dexamethasone reduced the 28-day mortality rate by 17% (rate ratio 0.83 [95% CI: 0.74 to 0.92]; P=0.0007). This is a big deal. 7/ 
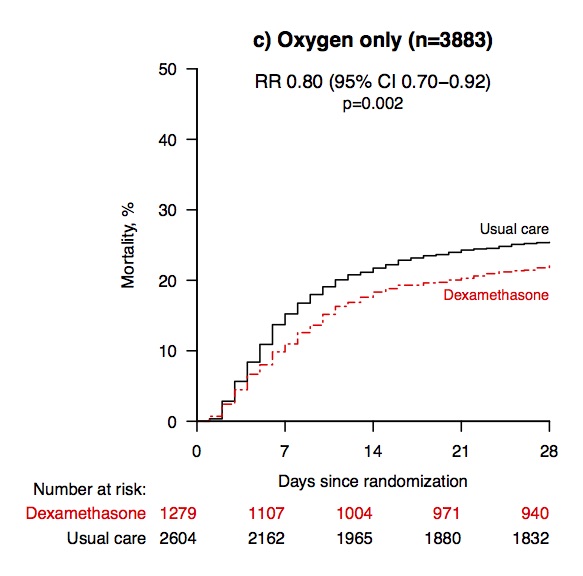
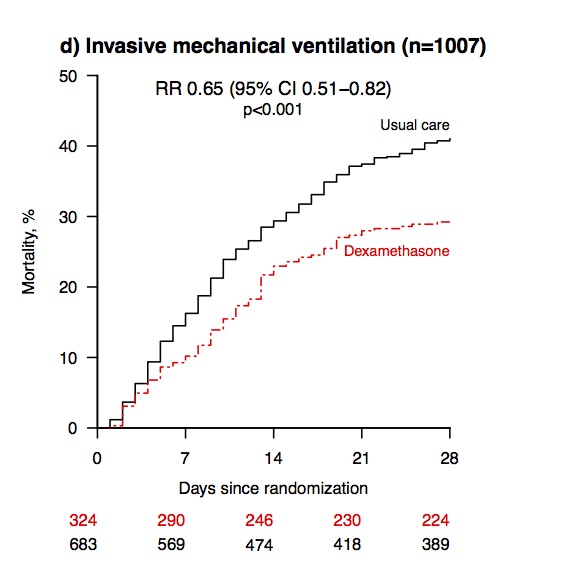
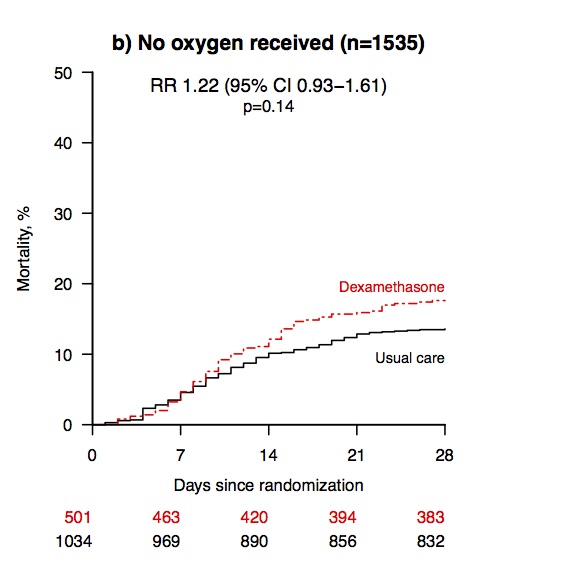
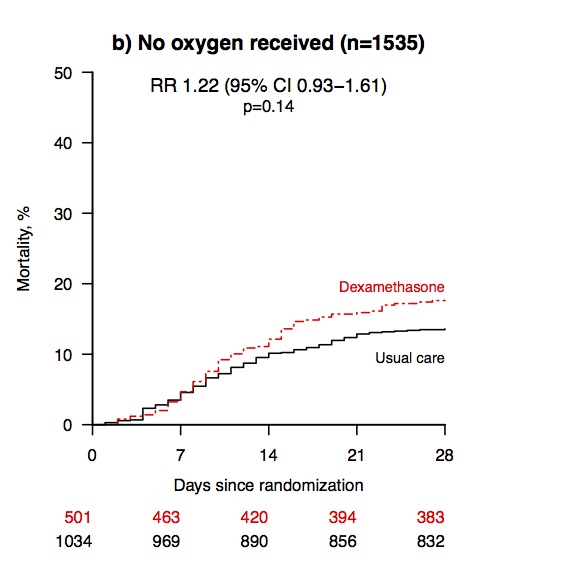
Among the patients who received usual care, 28-day mortality was highest in those patients who required ventilation at the outset (41%), intermediate in those who just required oxygen (25%), and lowest in those who did not require any respiratory help (13%). 8/
Dexamethasone reduced deaths by one-third in ventilated patients (rate ratio 0.65 [95% CI: 0.48 to 0.88]; p=0.0003)! And by one fifth in the patients receiving oxygen only (0.80 [0.67 to 0.96]; p=0.0021). 9/
There was no benefit among those patients who did not require respiratory support (1.22 [0.86 to 1.75; p=0.14).
Also important: the study did not study patients *outside* the hospital setting (e.g., who were not so sick). So don't pop dex. 10/
Also important: the study did not study patients *outside* the hospital setting (e.g., who were not so sick). So don't pop dex. 10/
There was a highly significant trend showing greatest benefit of dex among those COVID19 patients requiring more ventilator support (test for trend p<0.001). The sicker the patient was, the more the benefit of dex. 11/
The use of such steroid anti-inflammatory agents (e.g., dexamethasone) makes clinical sense. Such agents suppress our immune response, and many of the more lethal forms of COVID-19 arise not from the virus itself, but rather from an immune over-reaction to the virus. 12/
Hyper-induction of inflammatory mediators (“cytokine storm”) can cause diffuse damage to the alveoli at the end of the bronchi in our lungs, which is where oxygen exchange takes place. CT scans have shown (bad) typical changes (e.g., "bronchiolitis obliterans"). 13/
During the 2003 SARS pandemic, the clinical impression was that pulsed steroids sometimes produced a dramatic response. But the apparent benefits of steroids had proven to be incorrect before, as in case of infections with respiratory syncytial virus. link.springer.com/content/pdf/10… 14/
On the other hand, patients infected with a pathogen still need a fully functioning immune system to fend off the virus itself!
So an important issue is *which* patients should get dexamethasone and *when* in the course of their illness? 15/
So an important issue is *which* patients should get dexamethasone and *when* in the course of their illness? 15/
Indeed, there is a hint in the RCT that patients who did *not* require ventilators did *worse* on dex, supporting this concern.
For patients with illness not primarily from an immune over-reaction, giving dex might harm them, *increasing* risk of death by 22% (but p=0.14). 16/
For patients with illness not primarily from an immune over-reaction, giving dex might harm them, *increasing* risk of death by 22% (but p=0.14). 16/
On the issue of *when* in the course of COVID19 to use dex, it might make sense to wait until day ~6 of hospitalization. In essence, why run the risk of giving steroids if patient will not be one whose immune system over-reacts? 17/
It is likely that beneficial effect of dex in severe viral respiratory infections is dependent on using right dose, at right time, in right patient. It could be harmful, especially if given at a time when control of viral replication is paramount and inflammation is minimal. 18/
So, dexamethasone is a valuable treatment for serious COVID-19, as shown by this large, well conducted RCT. medrxiv.org/content/10.110… 19/
But this new trial highlights some other ongoing topics related to the COVID-19 pandemic. Let's talk about these, too. 20/
First, the dex RCT demonstrates how many modern RCT’s are done: “The protocol combines the methods of large, simple trials of treatments for acute myocardial infarction in the 1980s with the opportunities provided by digital health care in the 2020s.” 21/
Second, the dex RCT demonstrates how trials can be completed & publicized rapidly in modern era! “These preliminary results for dexamethasone were announced on 16 June 2020, just 98 days after protocol was first drafted, and were adopted into UK practice later the same day”! 22/
Here is the press release dated June 16 ox.ac.uk/news/2020-06-1…). And the paper was posted June 22. It is now undergoing full peer review and will no doubt be published in coming months. 23/
People are understandably a bit wary of putting too much confidence in rapidly emerging studies, given the issues with the retracted chloroquine studies. 24/
But it would be unethical to delay release of the results (which would appear lifesaving) to go through usual publication procedures for such a well-conducted study (though authors will surely publish their paper, in due course). [thread continues] 25/
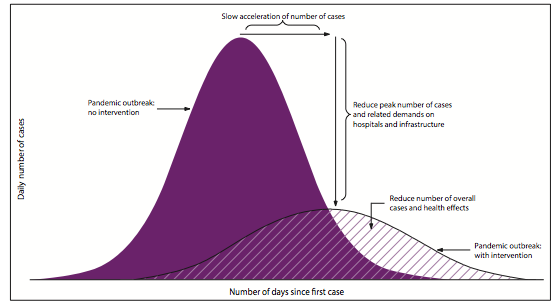
Third, the dex RCT provides a powerful illustration of the whole point of flattening the curve. We flattened the curve so as to allow medical science to find better ways to care for sick patients. And we are achieving that now! 26/
The remdesivir trial announced on April 29, 2020 was shown to shorten time to recovery, but not necessarily lower mortality: nih.gov/news-events/ne… 27/
Fourth, many people have wondered whether the seeming decline in overall lethality of SARS-CoV-2 in the USA nowadays might relate to the availability of better treatments and greater experience among doctors in how to care of patients (as with the foregoing drugs). 28/
I think that better medical care is only a small part of the decline, however.
I think primary reason COVID19 CFR is declining is younger average age of people currently getting the virus (which is much deadlier in older patients than young ones – ). 29/
I think primary reason COVID19 CFR is declining is younger average age of people currently getting the virus (which is much deadlier in older patients than young ones – ). 29/