
Do you often check a FeNa when working up a patient with AKI?
In my experience it’s ordered reflexively
But is this a good idea? Is a FeNa actually useful?
Let’s find out #NSMCInternship #nephtwitter #tweetorial
Poll!
To differentiate between prerenal AKI and ATN you would
In my experience it’s ordered reflexively
But is this a good idea? Is a FeNa actually useful?
Let’s find out #NSMCInternship #nephtwitter #tweetorial
Poll!
To differentiate between prerenal AKI and ATN you would
In normal circumstances sodium excretion = dietary intake
🔥What goes in must come out = extracellular volume is maintained within a narrow range
⬇️Volume → ⬆️RAAS →⬇️sodium excretion
⬆️Volume → ⬆️ANP → ⬆️sodium excretion
🤷♂️So why not just use UNa as a surrogate?
🔥What goes in must come out = extracellular volume is maintained within a narrow range
⬇️Volume → ⬆️RAAS →⬇️sodium excretion
⬆️Volume → ⬆️ANP → ⬆️sodium excretion
🤷♂️So why not just use UNa as a surrogate?
💡Remember UrNa is affected by concentration (hint: units are mEq/L)
Dilute urine = ⬇️UNa even if excretion is high
Concentrated urine = ⬆️UNa even if total excretion is low
🔥FeNa provides a measure of sodium handling that is INDEPENDENT of urinary concentration
Dilute urine = ⬇️UNa even if excretion is high
Concentrated urine = ⬆️UNa even if total excretion is low
🔥FeNa provides a measure of sodium handling that is INDEPENDENT of urinary concentration
FeNa Fact: First described in 1976 by Espinel
17 patients with oliguric AKI
Established current criteria:
<1% for pre-renal
>3% for acute tubular injury (in between values are considered indeterminate)
👉 Read the original article jamanetwork.com/journals/jama/…
17 patients with oliguric AKI
Established current criteria:
<1% for pre-renal
>3% for acute tubular injury (in between values are considered indeterminate)
👉 Read the original article jamanetwork.com/journals/jama/…
Premise:
💥⬇️Volume→neurohumoral activation→⬆️sodium reabsorption=⬇️excretion
💥Tubular injury→⬇️number of functional nephrons to excrete sodium load=⬆️FeNa
💥If GFR didn't ⬇️with impaired tubular absorption= kidney catastrophe (hence oliguria)
👉amjmed.com/article/0002-9…
💥⬇️Volume→neurohumoral activation→⬆️sodium reabsorption=⬇️excretion
💥Tubular injury→⬇️number of functional nephrons to excrete sodium load=⬆️FeNa
💥If GFR didn't ⬇️with impaired tubular absorption= kidney catastrophe (hence oliguria)
👉amjmed.com/article/0002-9…
Let’s💡about these numbers. What’s my FeNa right now?
Assume I have a normal GFR of 125 mL/min➕SNa of 140 mEq/L
I’m filtering 180L/d x 140 mEq/L=25k mEq/d of sodium
If I ingest 4g of sodium=172 mEq MY FeNa is 0.68%
But I feel fine, and don’t need a bolus, I don’t think..🤷♂️
Assume I have a normal GFR of 125 mL/min➕SNa of 140 mEq/L
I’m filtering 180L/d x 140 mEq/L=25k mEq/d of sodium
If I ingest 4g of sodium=172 mEq MY FeNa is 0.68%
But I feel fine, and don’t need a bolus, I don’t think..🤷♂️
For my FeNa to be >3% (assuming my dietary intake stays constant) I would need to reduce my GFR to at most 28 mL/min.
Therefore the APPLICATION of this formula is contingent on a patient having significant AKI
Therefore the APPLICATION of this formula is contingent on a patient having significant AKI
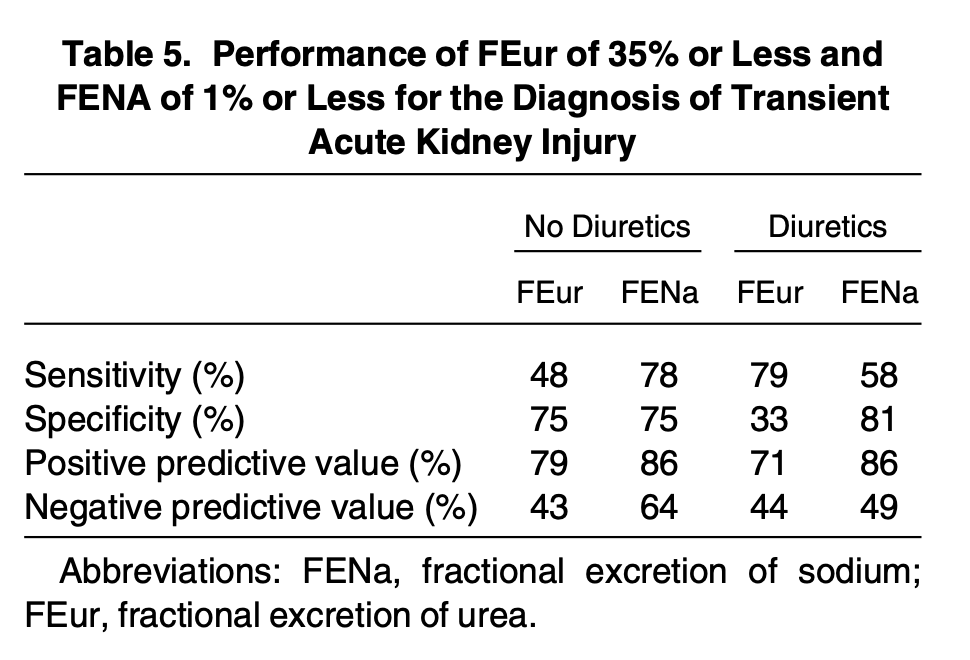
Subsequent studies have shown variable levels of performance as shown with its sensitivity and specificity in the below table 👇
🔥It tends to consistently test well in prerenal patients who are oliguric
🔥It tends to consistently test well in prerenal patients who are oliguric

Patient on diuretics? No problem get a FeUrea right?
Same principle as FeNa but urea primarily reabsorbed in the proximal tubule=unaffected by traditional (loop and thiazide) diuretics
Volume depletion=⬆️urea reabsorption=classic 20:1 BUN to creatinine ratio in a prerenal state
Same principle as FeNa but urea primarily reabsorbed in the proximal tubule=unaffected by traditional (loop and thiazide) diuretics
Volume depletion=⬆️urea reabsorption=classic 20:1 BUN to creatinine ratio in a prerenal state

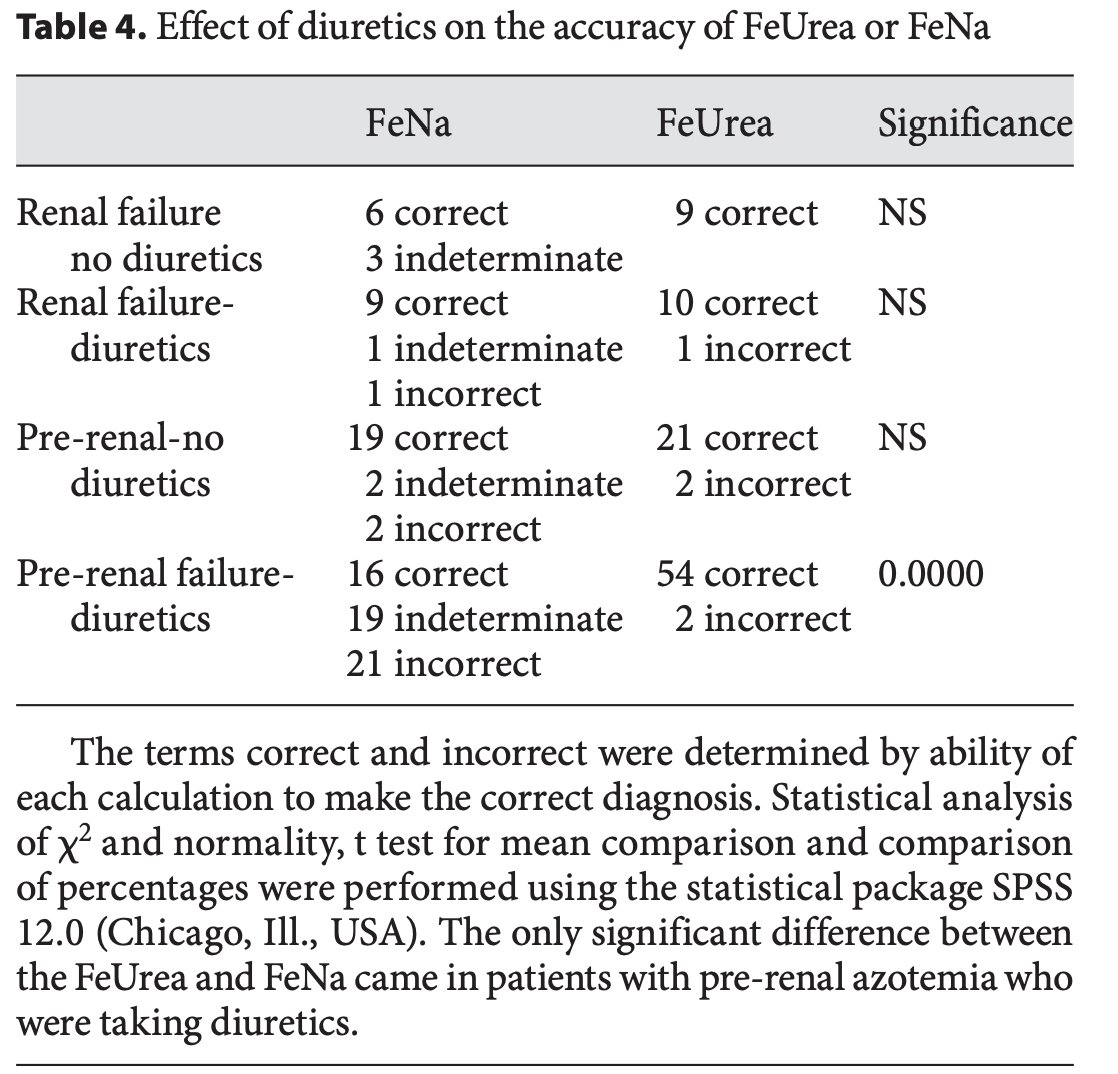
FeUrea Fact: 🥇 described by Kaplan and Kohn in 1992
💥Retrospective review
-87 patients,40 with discordant FeNa and FeUrea results,39 treated with diuretics
💥Similar efficacy in prerenal pts w/o diuretics but FeUrea>>FeNa in prerenal pts w/diuretics
👉…rger-com.offcampus.lib.washington.edu/Article/Abstra…
💥Retrospective review
-87 patients,40 with discordant FeNa and FeUrea results,39 treated with diuretics
💥Similar efficacy in prerenal pts w/o diuretics but FeUrea>>FeNa in prerenal pts w/diuretics
👉…rger-com.offcampus.lib.washington.edu/Article/Abstra…
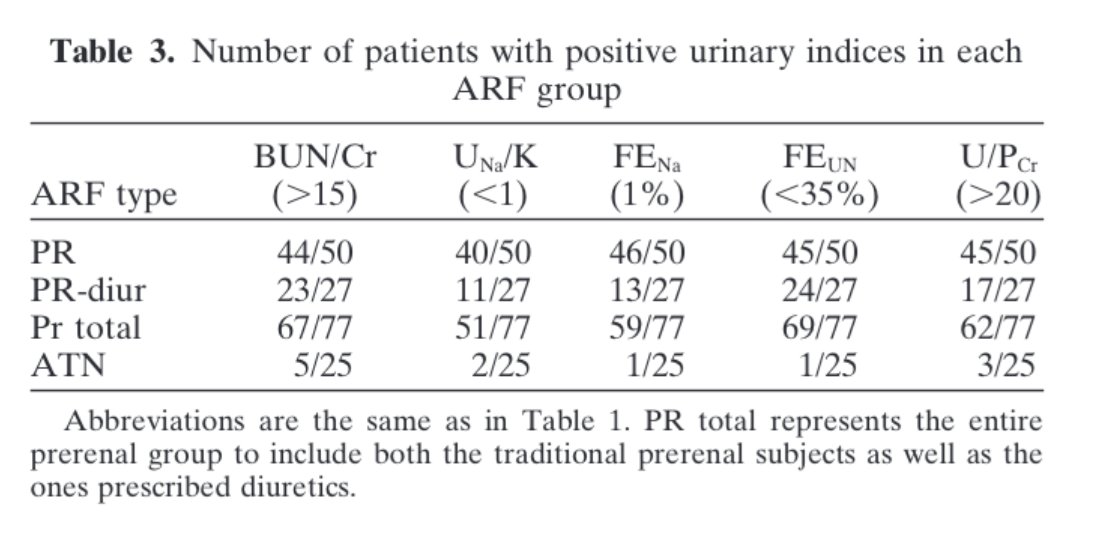
Is FeUrea effective?
💥Consistently beats FeNa in pts on diuretics, with variable overall efficacy
💥See tables 👇
💥Exception: FeNa outperformed FeUrea in septic patients
Why? Cytokine stimulation decreases urea excretion by ⬇️urea transporters
👉 journals.physiology.org/doi/pdf/10.115…
💥Consistently beats FeNa in pts on diuretics, with variable overall efficacy
💥See tables 👇
💥Exception: FeNa outperformed FeUrea in septic patients
Why? Cytokine stimulation decreases urea excretion by ⬇️urea transporters
👉 journals.physiology.org/doi/pdf/10.115…
So why such variability in performance with both tests?
💥The key is patient selection
💥There are a large number of factors that limit utility for both tests, many of which are common conditions in hospitalized patients, as shown 👇
💥The key is patient selection
💥There are a large number of factors that limit utility for both tests, many of which are common conditions in hospitalized patients, as shown 👇


So is there a better way?
This paper:
👉…nals-org.offcampus.lib.washington.edu/content/clinja…
looked at the utility of urine microscopy in differentiating between prerenal AKI and ATN with impressive likelihood ratios from the presence or absence of granular casts/renal tubular epithelial cells
This paper:
👉…nals-org.offcampus.lib.washington.edu/content/clinja…
looked at the utility of urine microscopy in differentiating between prerenal AKI and ATN with impressive likelihood ratios from the presence or absence of granular casts/renal tubular epithelial cells
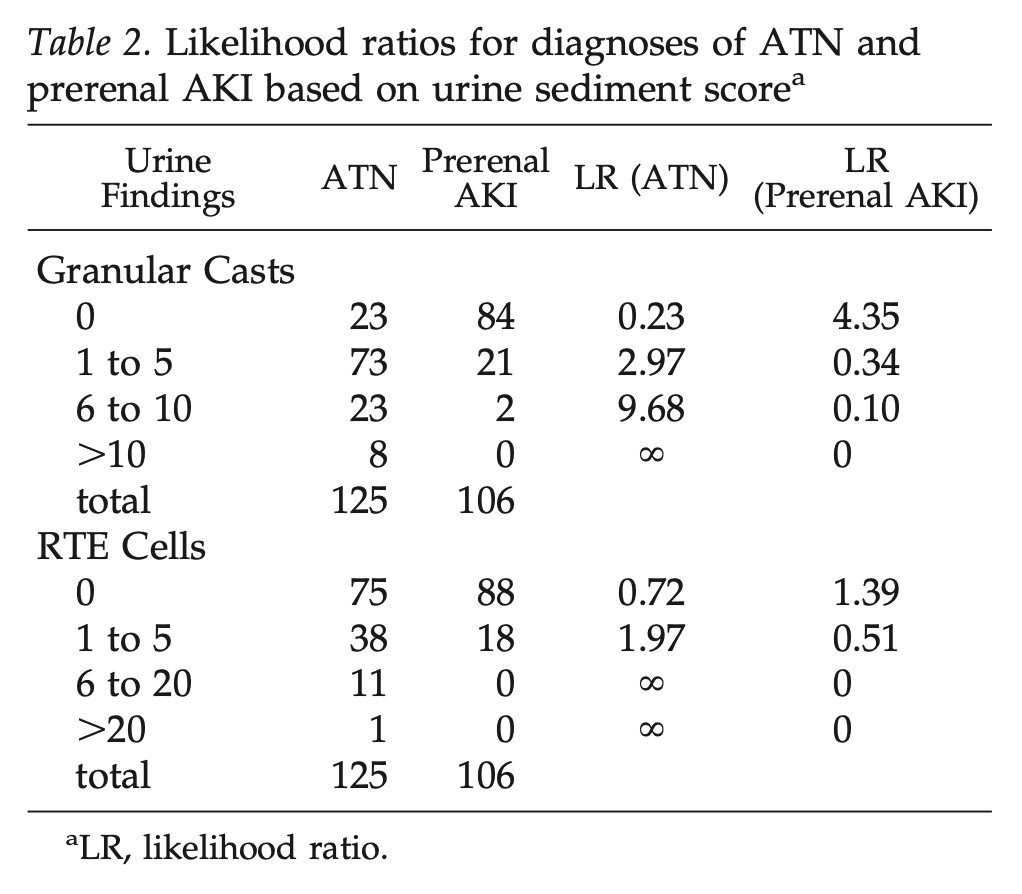
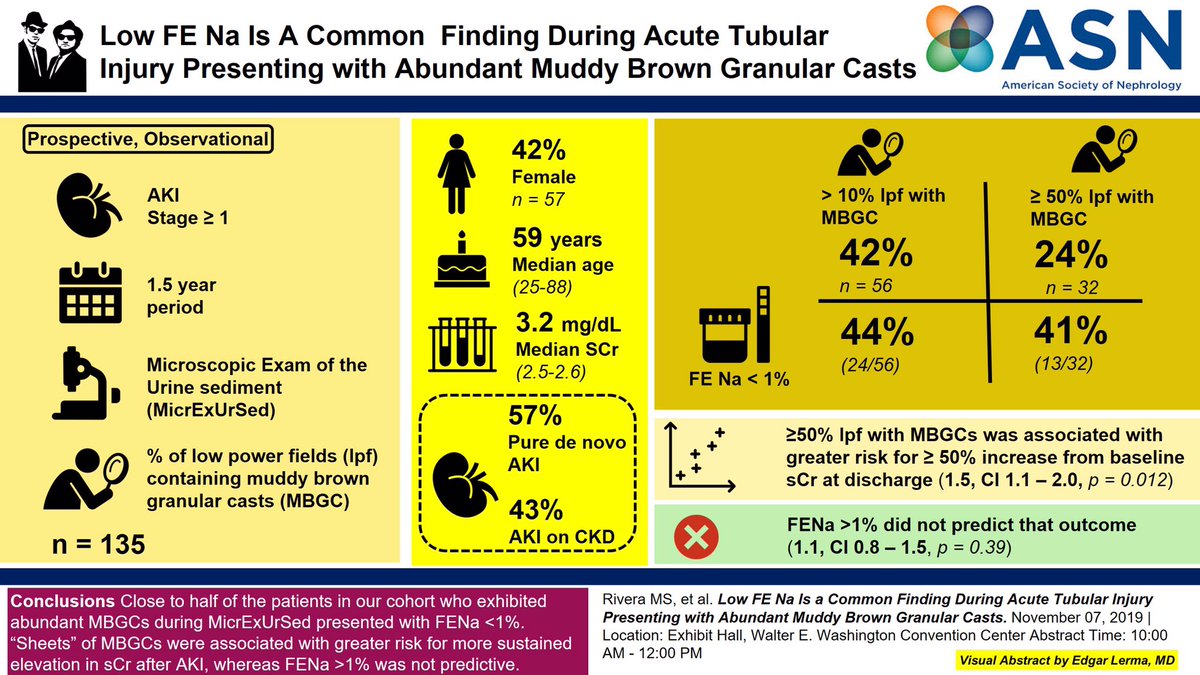
🔥This study found that a low FeNa (<1%) was common in patients with abundant muddy brown casts on microscopy.
Image courtesy of @edgarvlermamd
Image courtesy of @edgarvlermamd
Does this change your opinion?
The poll again:
To differentiate between prerenal AKI and ATN would you
The poll again:
To differentiate between prerenal AKI and ATN would you
Conclusion
💥FeNa MAY be useful in highly selected patients if <1%
💥>3% - who knows 🤷♂️
💥Either way - shouldn't be ordered as a knee jerk in every patient with AKI
💡 in these studies ATN/pre-renal were differentiated by rapidity of correction, often after volume repletion!
💥FeNa MAY be useful in highly selected patients if <1%
💥>3% - who knows 🤷♂️
💥Either way - shouldn't be ordered as a knee jerk in every patient with AKI
💡 in these studies ATN/pre-renal were differentiated by rapidity of correction, often after volume repletion!

