
2 years of Cardiology Fellowship in the books and officially done with consult services as a fellow. It's time for some 🫀 themed #tipsfornewdocs covering: Acute Coronary Syndrome💔Atrial Fibrillation🤦♂️ Cardiogenic 🆘 Shock⚡️ ; VT〰️, 💗 Failure(Diuretics🚰).
1/20 💔Chest Pain #tipsfornewdocs
☑️Know everything about patient's symptom before calling us. (Focused H&P) 🛑Is the patient having chest pain now?
☑️Review yourself (Trust but Verify) prior ECG and new ECG (during chest pain).
☑️Make Pain Go away: Start w/ Nitroglycerin sl.
☑️Know everything about patient's symptom before calling us. (Focused H&P) 🛑Is the patient having chest pain now?
☑️Review yourself (Trust but Verify) prior ECG and new ECG (during chest pain).
☑️Make Pain Go away: Start w/ Nitroglycerin sl.
2/20 💔Chest Pain #tipsfornewdocs
☑️Troponin should be cooking; Have available information regarding PLT; H/H; Creatinine; INR/PT
☑️Good to go for a discussion with the cardiology consultant.
☑️Troponin should be cooking; Have available information regarding PLT; H/H; Creatinine; INR/PT
☑️Good to go for a discussion with the cardiology consultant.
3/20 💔Troponin #tipsfornewdocs
Other non-cardiac reasons to have an elevated Troponin:
1⃣Critically ill patients, respiratory failure or sepsis
2⃣Acute neurological disease
3⃣Renal failure
4⃣Drug toxicity or toxins
5⃣Burns affecting >25 percent of BSA
6⃣Exertion
Other non-cardiac reasons to have an elevated Troponin:
1⃣Critically ill patients, respiratory failure or sepsis
2⃣Acute neurological disease
3⃣Renal failure
4⃣Drug toxicity or toxins
5⃣Burns affecting >25 percent of BSA
6⃣Exertion
4/20 🤦♂️A-FIB #tipsfornewdocs
☑️Patient intubated/shock(septic) on multiple pressors is found to be in Atrial Fibrillation with RVR 🛑 Correct Underlying Acute Illness (Treat Sepsis)
☑️Patient admitted for CHF, found to in AF with RVR 🛑 Treat CHF 🚰
☑️Patient intubated/shock(septic) on multiple pressors is found to be in Atrial Fibrillation with RVR 🛑 Correct Underlying Acute Illness (Treat Sepsis)
☑️Patient admitted for CHF, found to in AF with RVR 🛑 Treat CHF 🚰
5/20 💗Failure #tipsfornewdocs
Things to know before calling a HF consult:
1⃣ Is patient cold+wet; warm+wet; cold+dry; cold+wet?
2⃣ Etiology of heart failure? Cause of decompensation?
3⃣ Left Ventricular Function: Reduced LVEF or Preserved?
4⃣ Outpatient Medical Regimen?
Things to know before calling a HF consult:
1⃣ Is patient cold+wet; warm+wet; cold+dry; cold+wet?
2⃣ Etiology of heart failure? Cause of decompensation?
3⃣ Left Ventricular Function: Reduced LVEF or Preserved?
4⃣ Outpatient Medical Regimen?
6/20 💗Failure #tipsfornewdocs
✖️Do not administer beta-blockers or calcium channel blockers to a patient with acute decompensated heart failure(ADHF). (ie: Treat acute HF , not atrial fibrillation)
✔️Continue with beta-blockers in ADHF if patients is allready on them.
✖️Do not administer beta-blockers or calcium channel blockers to a patient with acute decompensated heart failure(ADHF). (ie: Treat acute HF , not atrial fibrillation)
✔️Continue with beta-blockers in ADHF if patients is allready on them.
7/20 💗Failure #tipsfornewdocs
✔️In a Wet HF w/ AKI->(Diuresis is almost always the answer🚰.
✔️Don't stop ACEi/ARB in HFrEF with AKI
✔️Don't stop Beta-blockers unless in SHOCK.
✔️Look to make progress!
✔️Get with the guidelines; Remember Guideline Directed Medical Therapy!!!
✔️In a Wet HF w/ AKI->(Diuresis is almost always the answer🚰.
✔️Don't stop ACEi/ARB in HFrEF with AKI
✔️Don't stop Beta-blockers unless in SHOCK.
✔️Look to make progress!
✔️Get with the guidelines; Remember Guideline Directed Medical Therapy!!!
8/20 💗Failure #tipsfornewdocs
Document why patient is not on the following (better have a good reason cause they #GDMTwork):
☑️Beta-Blockers
☑️ACEi/ARB/ARNI
☑️Aldactone/Spironolactone
☑️SLG-1 inhibitors
☑️CRT
Document why patient is not on the following (better have a good reason cause they #GDMTwork):
☑️Beta-Blockers
☑️ACEi/ARB/ARNI
☑️Aldactone/Spironolactone
☑️SLG-1 inhibitors
☑️CRT
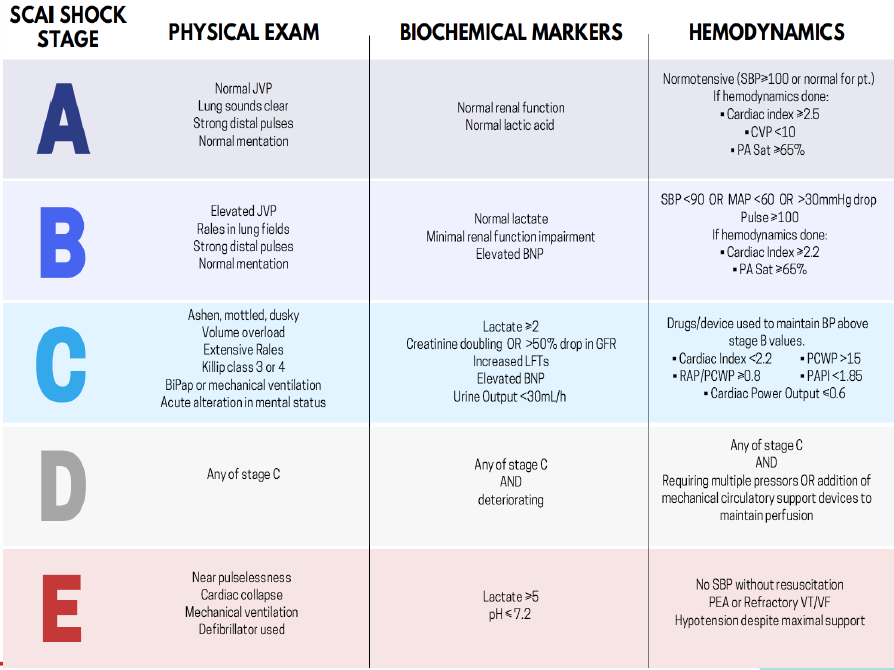
9/20 Cardiogenic 🆘 Shock⚡️ #tipsfornewdocs
☑️ Recognize sign of early Cardiogenic Shock -> Increase chance of recovery and prevents detrimental irreversible end-organ damage
☑️ Know your ABCs
☑️ Recognize sign of early Cardiogenic Shock -> Increase chance of recovery and prevents detrimental irreversible end-organ damage
☑️ Know your ABCs
10/20 Polymorphic VT 〰️ #Tipsfornewdocs
All Torsades de pointes are polymorphic VT but not all polymorphic VT are torsades de pointes.
🛑If you see polymorphic VT->Think of ischemia
All Torsades de pointes are polymorphic VT but not all polymorphic VT are torsades de pointes.
🛑If you see polymorphic VT->Think of ischemia
11/20 Pericardial Tamponade #tipsfornewdocs
Not all pericardial effusion -> pericardial tamponade
1⃣Like heart failure, It remains a clinical diagnosis.
2⃣Know how to calculate Pulsus paradoxus (>12 mmHg)
Not all pericardial effusion -> pericardial tamponade
1⃣Like heart failure, It remains a clinical diagnosis.
2⃣Know how to calculate Pulsus paradoxus (>12 mmHg)
12/20 Consult to turn off ICD in a Comfort Measure Patient. #tipsfornewdocs
2 options.
1⃣Place a magnet over the ICD which will prevent an ICD discharge but does NOT turn off the pacemaker
2⃣Turn off Tachytherapies via device programmer.
2 options.
1⃣Place a magnet over the ICD which will prevent an ICD discharge but does NOT turn off the pacemaker
2⃣Turn off Tachytherapies via device programmer.
13/20 ⬆️BP causes #tipsfornewdocs
1⃣Apnea (obstructive sleep apnea), Accuracy (incorrect measurement)
2⃣Birth control, Bad kidney
3⃣Coarctation of the aorta
4⃣Drugs
5⃣Endocrine disorders, erythropoietin
6⃣Fibromuscular dysplasia
1⃣Apnea (obstructive sleep apnea), Accuracy (incorrect measurement)
2⃣Birth control, Bad kidney
3⃣Coarctation of the aorta
4⃣Drugs
5⃣Endocrine disorders, erythropoietin
6⃣Fibromuscular dysplasia
15/20 Tachycardia #TipsForNewDocs
Causes:
1⃣Pain
2⃣Hypovolemia (Acute Blood Loss; Dehyration)
3⃣Infection
4⃣Pulmonary Embolism
5⃣Myocardial Injury/Structural Heart Defect ✔️
Causes:
1⃣Pain
2⃣Hypovolemia (Acute Blood Loss; Dehyration)
3⃣Infection
4⃣Pulmonary Embolism
5⃣Myocardial Injury/Structural Heart Defect ✔️
16/20 If 🤦♂️A-FIB consider #tipsfornewdoc
1⃣Pulmonary embolism and Pulmonary disease.
2⃣Ischemic heart disease.
3⃣Structural Heart Disease
4⃣Anemia, alcohol and age.
5⃣Thyroid disease
6⃣Sleep apnea, sepsis & surgery
1⃣Pulmonary embolism and Pulmonary disease.
2⃣Ischemic heart disease.
3⃣Structural Heart Disease
4⃣Anemia, alcohol and age.
5⃣Thyroid disease
6⃣Sleep apnea, sepsis & surgery
17/20 Hyperlipidemia #TipsForNewDocs
Don't Forget there is always Rosuvastatin ! tell them @TheFunshul
🛑Rosuvastatin has the greatest LDL reduction and HDL raising of the HMG-CoA reductase inhibitors.
Don't Forget there is always Rosuvastatin ! tell them @TheFunshul
🛑Rosuvastatin has the greatest LDL reduction and HDL raising of the HMG-CoA reductase inhibitors.
18/20 Beta-Blockers #TipsForNewDocs
☑️Carvedilol and labetalol are non-selective beta-blockers that also block alpha-1 receptors.
Ok to use in the setting of cocaine
☑️Carvedilol and labetalol are non-selective beta-blockers that also block alpha-1 receptors.
Ok to use in the setting of cocaine
19/20 VT #TipsForNewDocs
☑️Treat a wide QRS complex tachycardia like ventricular tachycardia until proven otherwise.
For more, see 👇👇👇
☑️Treat a wide QRS complex tachycardia like ventricular tachycardia until proven otherwise.
For more, see 👇👇👇

20/20 Thank you for the consult, please page with any questions/concerns. #TipsForNewDocs

