Thread
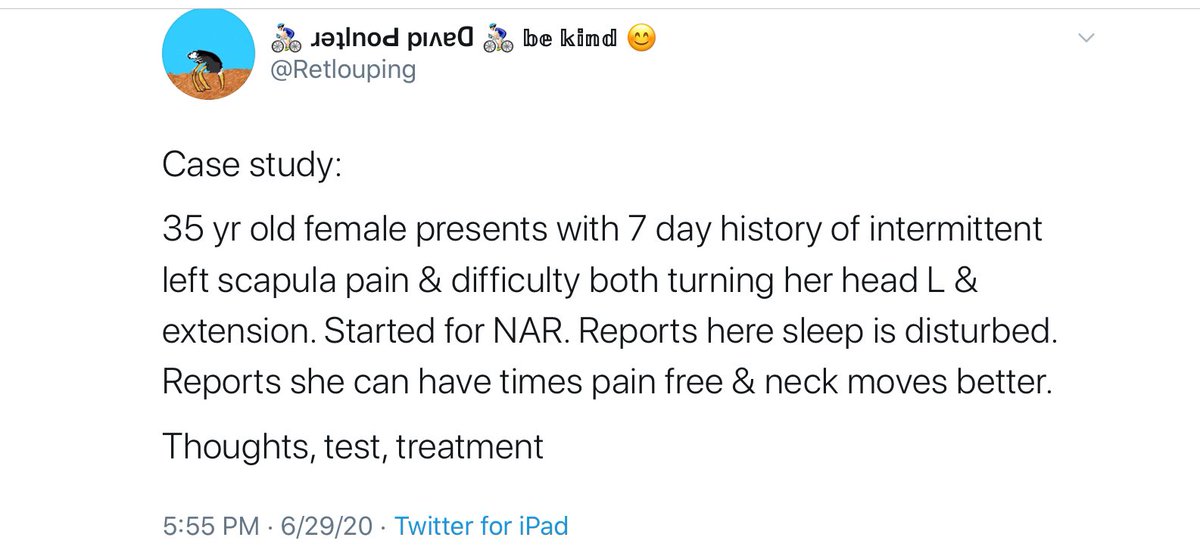
posted this case study yesterday. Several things happened.
1. People assumed there was a catch.
2. People thought It couldn’t be so straight forward.
3. People cautiously answered in the thread
So my intent was not to catch anyone out. My intent is to learn, with others
posted this case study yesterday. Several things happened.
1. People assumed there was a catch.
2. People thought It couldn’t be so straight forward.
3. People cautiously answered in the thread
So my intent was not to catch anyone out. My intent is to learn, with others
I am trying to provide a safe space to discuss and learn. I was upset by a DM I received from someone who posted the correct answer on a case study, but immediately deleted it. Fear of being challenged and or ridiculed on twitter. Seriously, what have we come to?
If we can’t openly share or thoughts inorder to learn and grow, then we have lost the plot as educators.
Time for a bit off self reflection.
If you are providing clinical education off SoMe, why are you creating a negative learning environment on SoMe.
YOU KNOW WHO YOU ARE.
Time for a bit off self reflection.
If you are providing clinical education off SoMe, why are you creating a negative learning environment on SoMe.
YOU KNOW WHO YOU ARE.
Rant over.
The case study was meant to be a run of the mill typical MSK patient, no red flags or serious emotional distress.
Intent, how do clinicians mange these patients on a daily basis.
The case study was meant to be a run of the mill typical MSK patient, no red flags or serious emotional distress.
Intent, how do clinicians mange these patients on a daily basis.
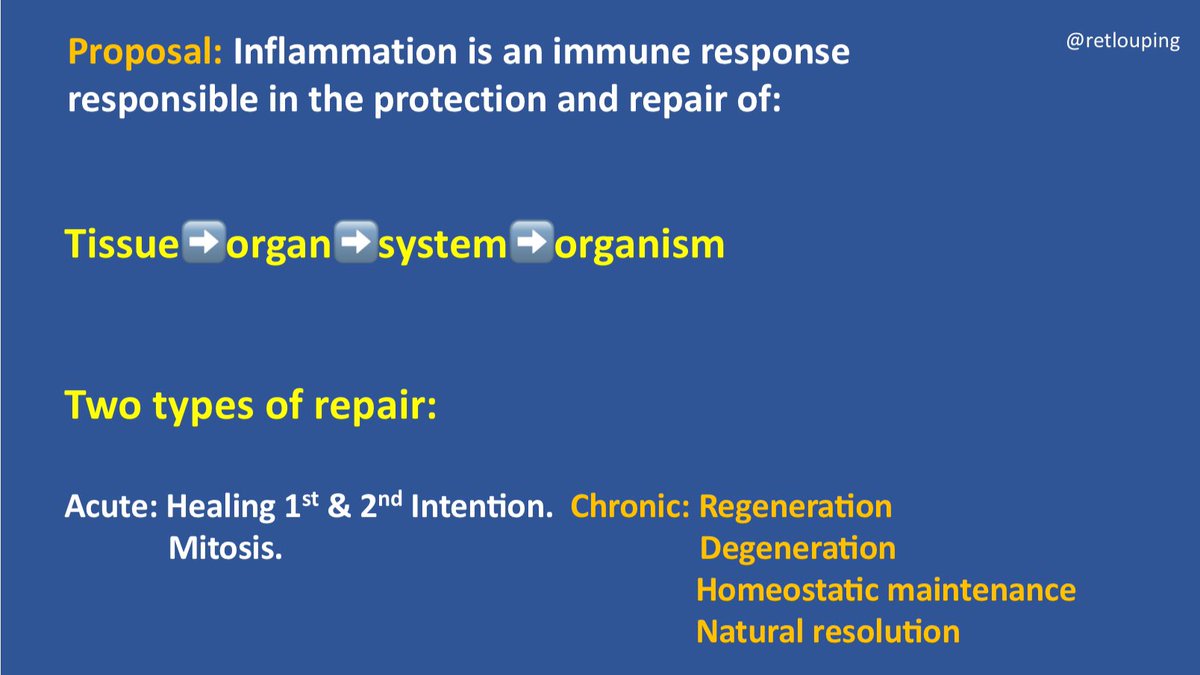
The patient presents with an acute episode of intermittent pain and neck stiffness. This is a typical somatic referred pattern from the cervical spine. Non nerve root or dura, no associated Neuro signs or symptoms.
The question is based on your Tx bias what Tx would she receive?
The question is based on your Tx bias what Tx would she receive?
That’s the rub. Given the same simple non complex presentation, would different clinicians do different treatments?
What did the patient expect?
Things we forget to,ask, previous history, has she had similar events, frequency, duration, intensity, distribution, medication.
What did the patient expect?
Things we forget to,ask, previous history, has she had similar events, frequency, duration, intensity, distribution, medication.
How long to recover from previous episode, of she had any.
What helped, what didn’t?
Is the current episode different, if so how?
What are the nature of her current signs and symptoms?
Frequency, duration, intensity, distribution, medication, any other interventions?
What helped, what didn’t?
Is the current episode different, if so how?
What are the nature of her current signs and symptoms?
Frequency, duration, intensity, distribution, medication, any other interventions?
Knowing why she is sat in front of us is key.
This was a real patient who I assisted with self treatment.
What I did with her really isn’t the issue, what you will do,with her is the important part.
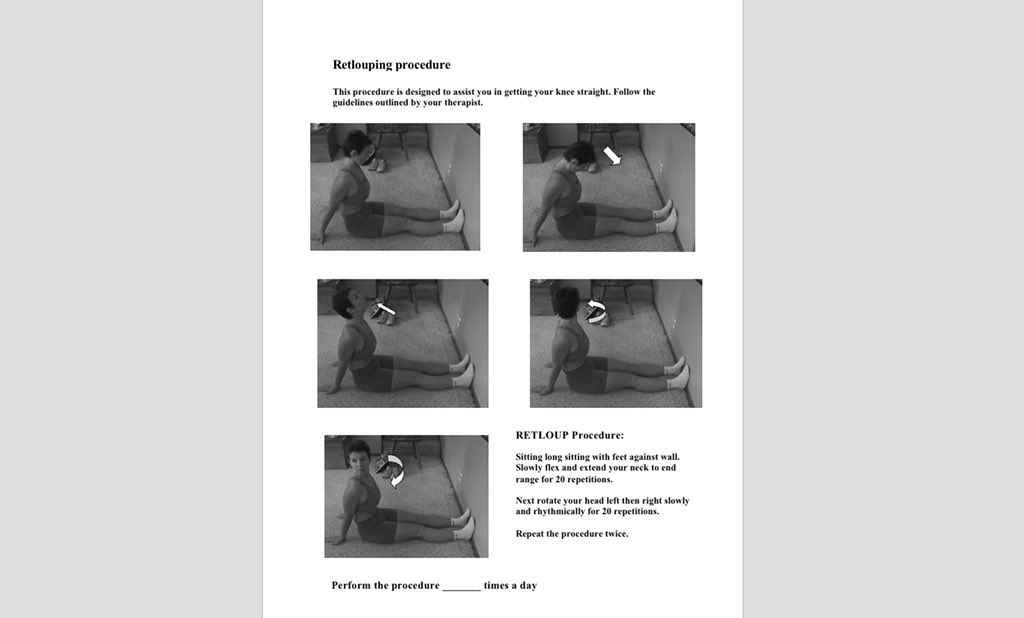
My bias is to find symptom and mechanical modification procedures.
This was a real patient who I assisted with self treatment.
What I did with her really isn’t the issue, what you will do,with her is the important part.
My bias is to find symptom and mechanical modification procedures.
Utilizing her own baselines and some symptom and movement loss baselines.
Allowing her to experience changes during and afterwards, under her own choice and control. Returning her locus of control internally and enhancing her self efficacy.
Allowing her to experience changes during and afterwards, under her own choice and control. Returning her locus of control internally and enhancing her self efficacy.
Thanks for the great contributions to the initial thread.
My process is outlined in this tweetorial, for what it is worth.
My process is outlined in this tweetorial, for what it is worth.
Let’s continue to create safe learning spaces. 😊