
Things to know if you work on medical ML:
- Medical data can be incomplete, incorrect, missing, & biased
- Medical system is disempowering & often traumatic for patients
- Crucial to involve patients & to recognize risk of how ML can end up further disempowering 1/
- Medical data can be incomplete, incorrect, missing, & biased
- Medical system is disempowering & often traumatic for patients
- Crucial to involve patients & to recognize risk of how ML can end up further disempowering 1/
On bias in medicine (& thus medical data): research shows that the pain of women is taken less seriously than pain of men. The pain of people of color is taken less seriously than pain of white people.
Result: longer time delays, lower quality of care, & worse outcomes 2/
Result: longer time delays, lower quality of care, & worse outcomes 2/
A meta-analysis of 20 years of published research found that Black patients were 22% less likely than whites to get *any* pain medication and 29% less likely to be treated with opioids 3/
bbc.com/future/article…
bbc.com/future/article…
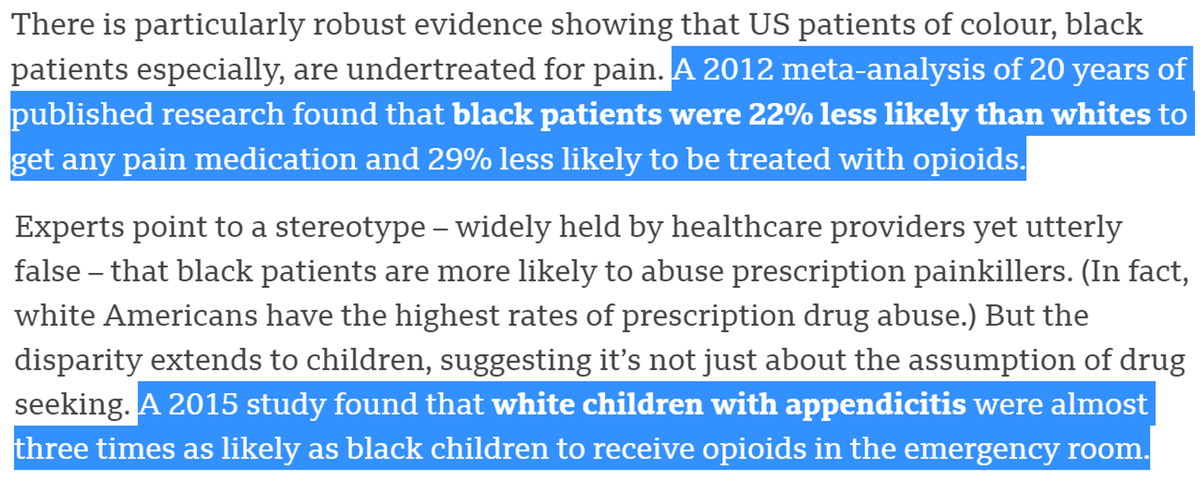
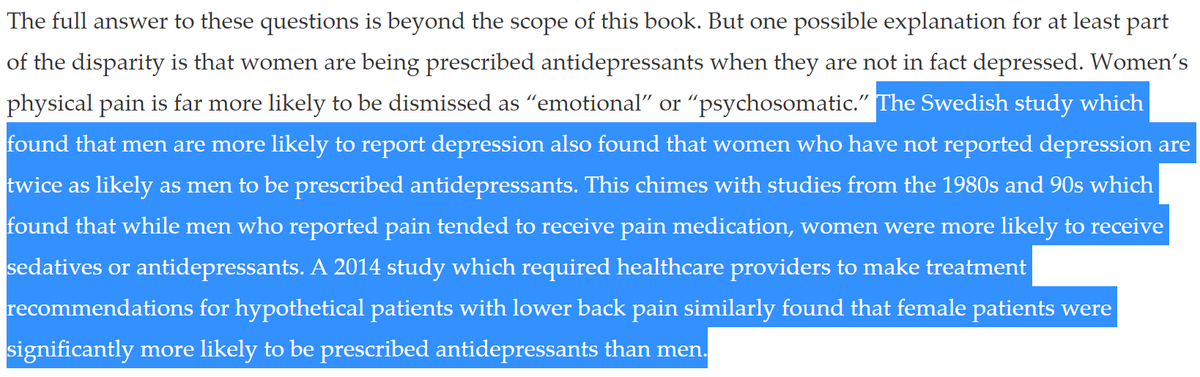
Men who report pain tend to receive pain medication, women who report pain are more likely to receive sedatives or antidepressants 4/
longreads.com/2019/06/21/yen…
also: bbc.com/future/article…
longreads.com/2019/06/21/yen…
also: bbc.com/future/article…
On average, it takes 5 years and 5 doctors for patients w/ autoimmune diseases (75% are women) to get a correct diagnosis
Diagnosis of Crohn's disease takes 12 months for men, 20 months for women
Diagnosis for Ehlers-Danlos syndrome takes 4 years for men, 16 years for women 5/
Diagnosis of Crohn's disease takes 12 months for men, 20 months for women
Diagnosis for Ehlers-Danlos syndrome takes 4 years for men, 16 years for women 5/
These diagnostic delays lead to incomplete, incorrect, & biased data at any one snapshot in time. How many additional patients get discouraged and give up? 6/
Links for tweet 5:
psmag.com/social-justice…
bbc.com/future/article…
Links for tweet 5:
psmag.com/social-justice…
bbc.com/future/article…
My knowledge of medical system is based in: personal experience (multiple surgeries, ICU stays, chronic illness), reading hundreds of patient accounts, & research on medical bias. I have also studied how ML can amplify harms in other complex systems with big power differences. 7/
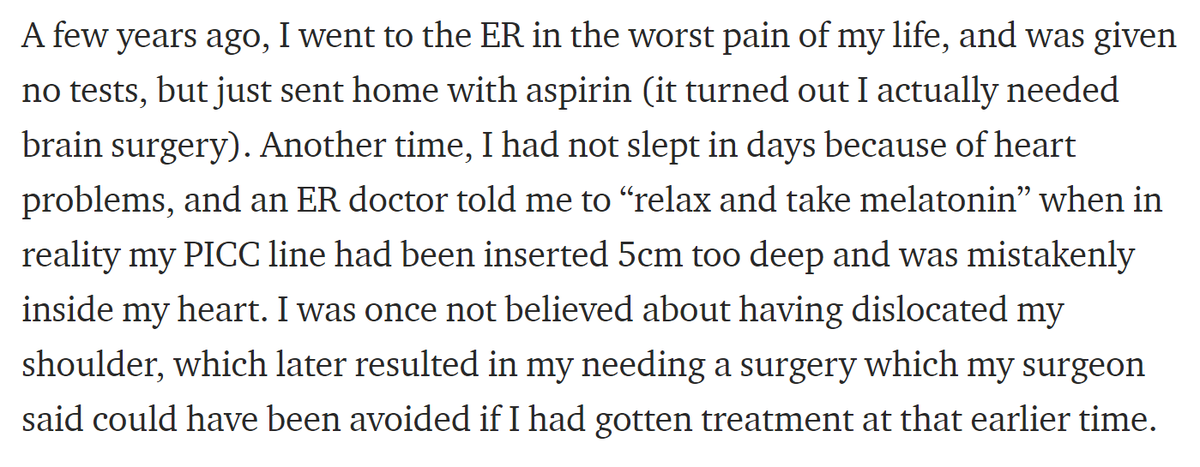
I wrote about some of my experiences of being disbelieved & dismissed, including the time I was sent home from the ER in terrible pain with no tests & only aspirin, but I actually needed brain surgery 8/
medium.com/@racheltho/the…
medium.com/@racheltho/the…
Read @aubreyhirsch's powerful comic on how it took her 6 years to get an accurate diagnosis due to being dismissed & disbelieved, during which time she developed permanent damage to her bones, eyes, & heart. Her account resonated with 100s. 9/
An algorithm to determine medicaid had a bug in the code, and incorrectly cut needed care for patients with cerebral palsy. There was no way to contest or appeal these decisions. 10/
theverge.com/2018/3/21/1714…
theverge.com/2018/3/21/1714…
Too often, ML has the effect of further concentrating & centralizing power, often unintentionally. I’m concerned about how that could amplify existing biases & harms in medicine, unless we are deliberate in using more participatory approaches. 11/
Algorithmic fairness & human-centered ML often focus on centralized solutions, lending increasing power to system designers & operators.
Participatory ML seeks more democratic, cooperative, & participatory systems. Please read this thread for more: 12/
Participatory ML seeks more democratic, cooperative, & participatory systems. Please read this thread for more: 12/
Question: do you know of any work at the intersection of medical ML and participatory ML? Please let me know! 13/
Domain expertise is crucial for any applied machine learning project. In the medical context, *domain expertise* must include doctors AND patients.
Patients have a set of skills and expertise that is distinct from doctors. 14/
Patients have a set of skills and expertise that is distinct from doctors. 14/
Patients are the experts on: what they are experiencing, how to navigate the medical system (doctors are often unaware of what this requires from the patient perspective), and how to advocate. 15/
As a patient, it is not your pain or symptoms that matter on their own, but the extent to which you can make them *legible* to the medical system.
Race, gender, class, weight, sexuality, & many other factors will impact your ability to do so, or what contortions may be required
Race, gender, class, weight, sexuality, & many other factors will impact your ability to do so, or what contortions may be required
The experience of knowing that something is very wrong with your body, and having a doctor write it off is frustrating & terrifying & unfortunately common. 17/
You can find plenty of online discussions of patient strategies that may be sadly necessary to try to receive care (e.g. around not mentioning anxiety, since doctors will write off your other problems, or on only naming 4 top symptoms, to avoid being labeled a hypochondriac) 18/
I have learned to develop an “elevator pitch” highlighting key issues, why they are important, & most relevant parts of my history-- to not expect that doctors have time to keep track of anything else, synthesize larger amounts of info, nor remember any previous conversation. 19/
It is also worth noting that many patients, particularly with rare or not widely understood illnesses, actively read medical papers, and in some cases will be more familiar with recent, relevant medical literature than some doctors. 20/




