flipping the vent! CPAP & APRV
- usually we dichotomize vent into 1st forcing patient to obey our tidal volumes, only later on allowing patients to breathe on their own
- CPAP/APRV: patient breathes on their own from the start
- @EMNerd_at #HRreloaded
- usually we dichotomize vent into 1st forcing patient to obey our tidal volumes, only later on allowing patients to breathe on their own
- CPAP/APRV: patient breathes on their own from the start
- @EMNerd_at #HRreloaded


to breathe, we need 3 things:
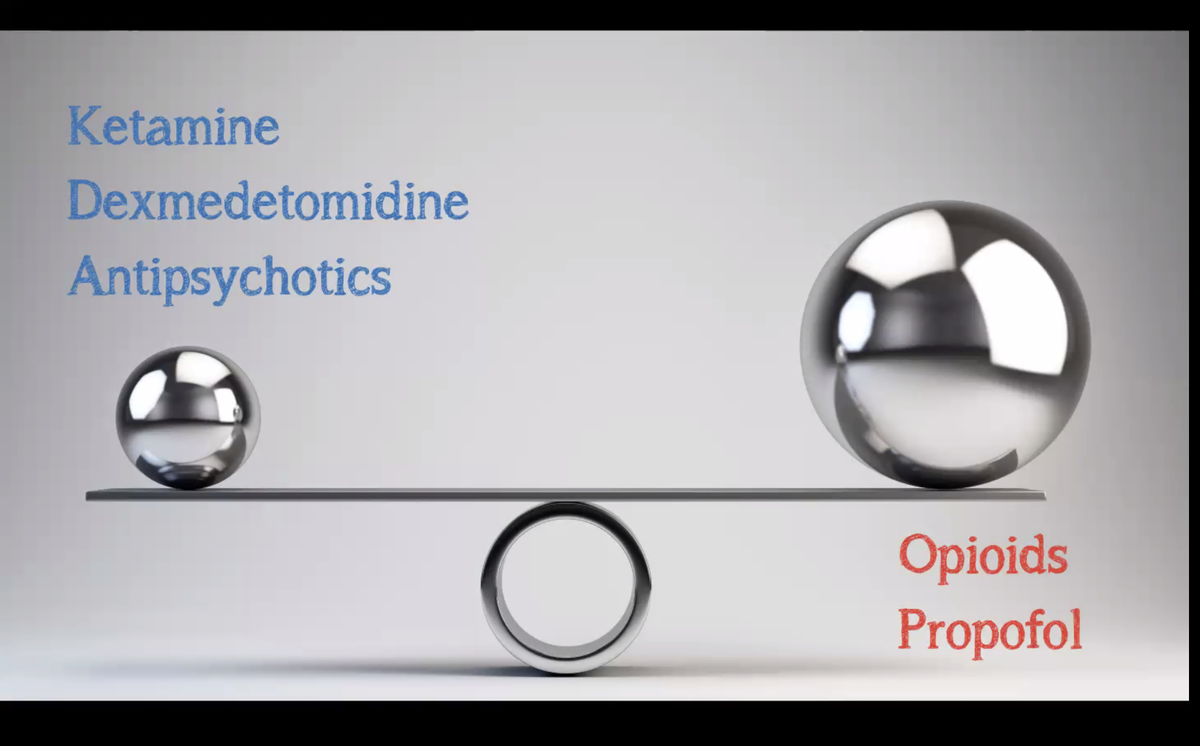
1) neurological drive to breathe (often depends on sedation and analgesia)
2) working diaphragm
3) adequate compliance
- @EMNerd_at #HRreloaded
1) neurological drive to breathe (often depends on sedation and analgesia)
2) working diaphragm
3) adequate compliance
- @EMNerd_at #HRreloaded
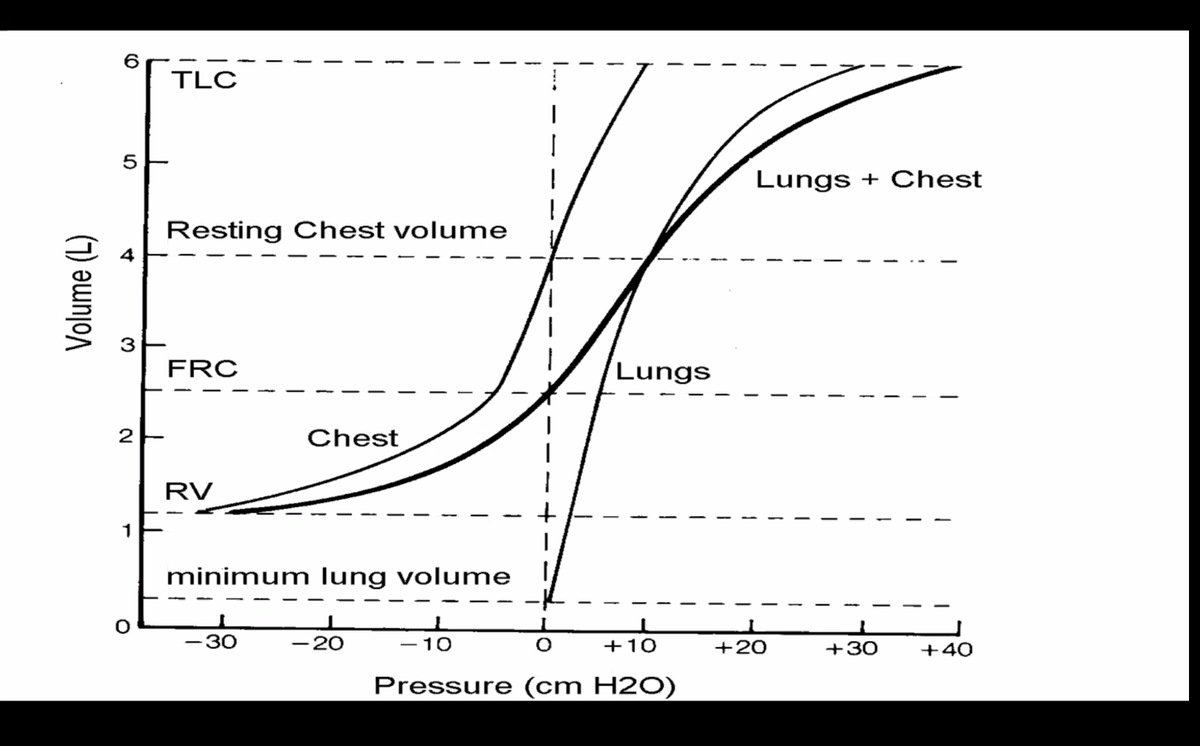
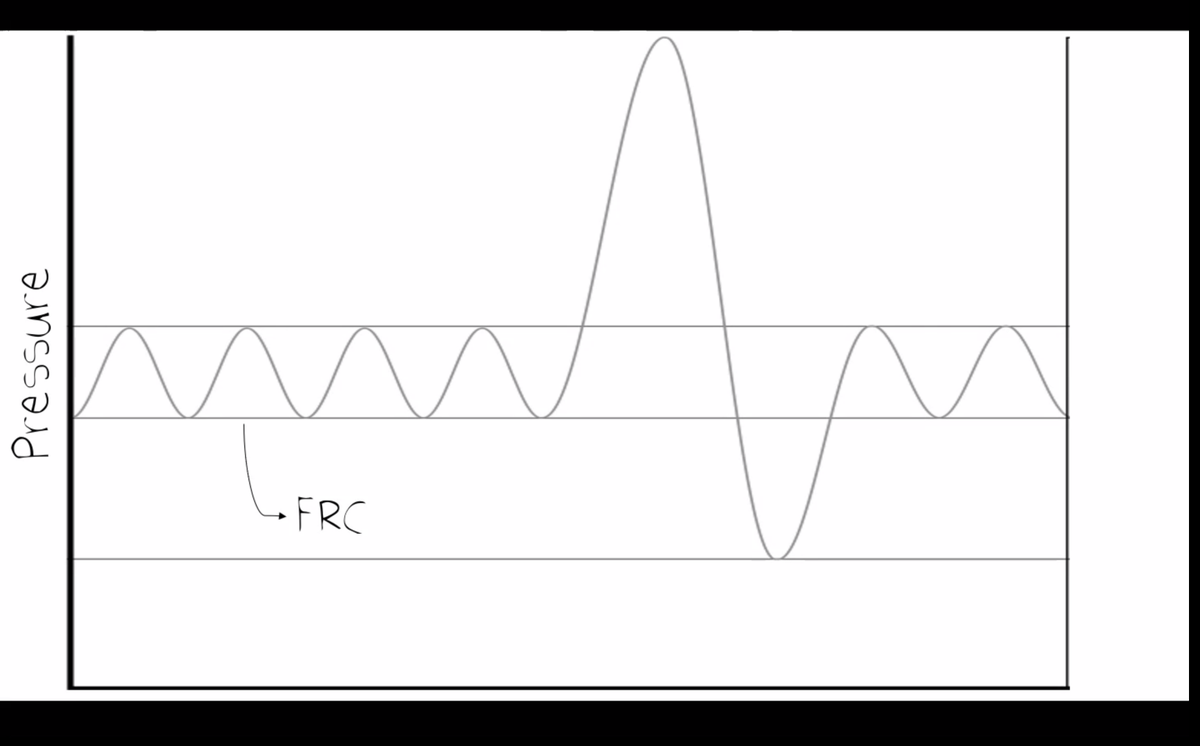
most patients have problems with #3 - patients are operating with a compressed "baby lung" which isn't at their normal residual volume. CPAP may bring the patient back to their resting lung volume, allowing the patient to breathe on their own.
- @EMNerd_at #HRreloaded
- @EMNerd_at #HRreloaded
early CPAP accelerates vent weaning by forcing patients to breathe throughout their ICU stay. this may naturally avoid over-sedation. balancing different analgesics & sedation may achieve an adequate respiratory drive
- @EMNerd_at #HRreloaded
- @EMNerd_at #HRreloaded
is the patient at their optimal end-tidal lung volume? over time, patients tend to de-recruit causing FRC to shrink. the key challenge with CPAP is what the optimal pressure is to inflate the lungs (without over-inflation).
- @EMNerd_at #HRreloaded
- @EMNerd_at #HRreloaded
If CPAP is too low, the lung may derecruit and the patient will start visibly failing (e.g. with rapid & shallow breathing).
- @EMNerd_at #HRreloaded
- @EMNerd_at #HRreloaded
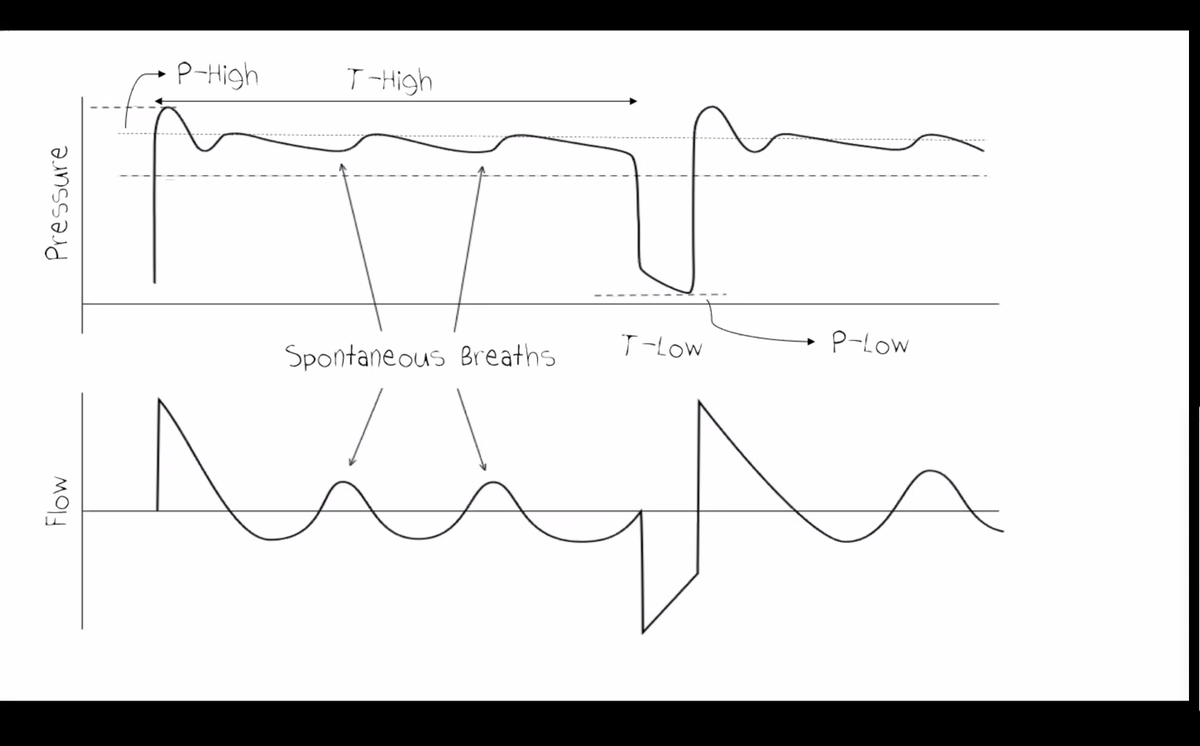
APRV may be used to provide some mechanical support while patients recover, if they are too sick initially to breathe on CPAP alone. the release metabolically off-loads CO2 as the patient improves.
- @EMNerd_at #HRreloaded
- @EMNerd_at #HRreloaded
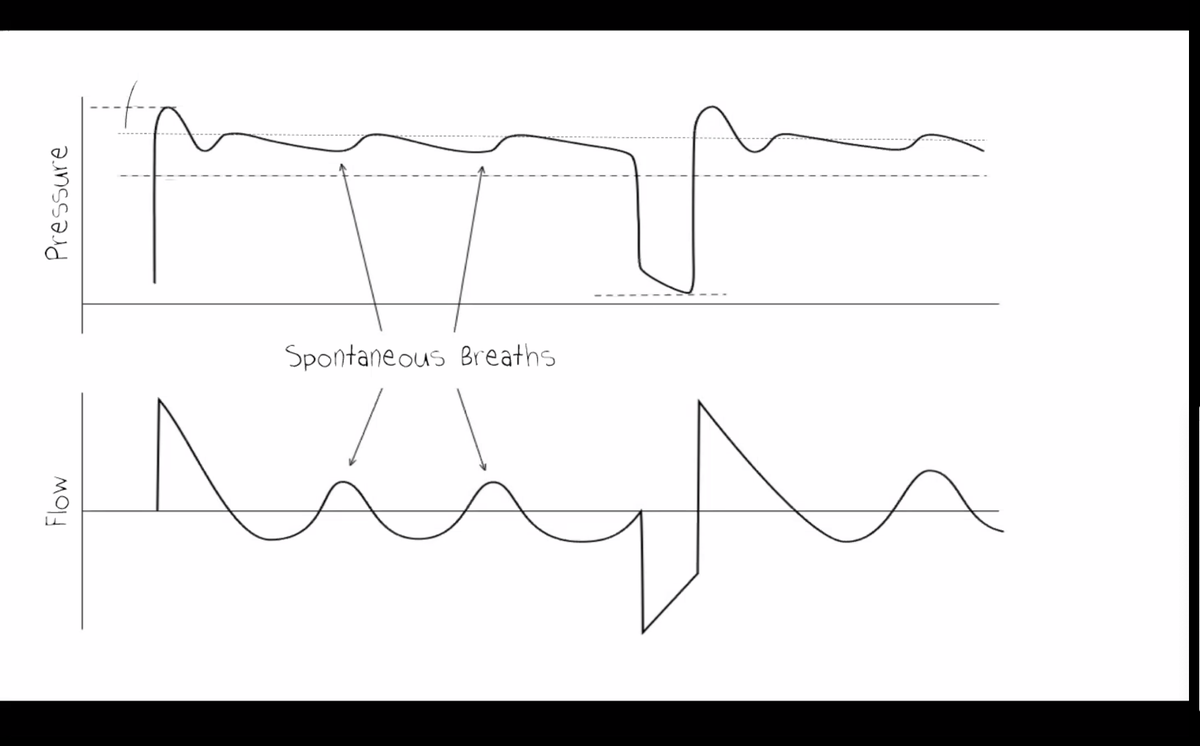
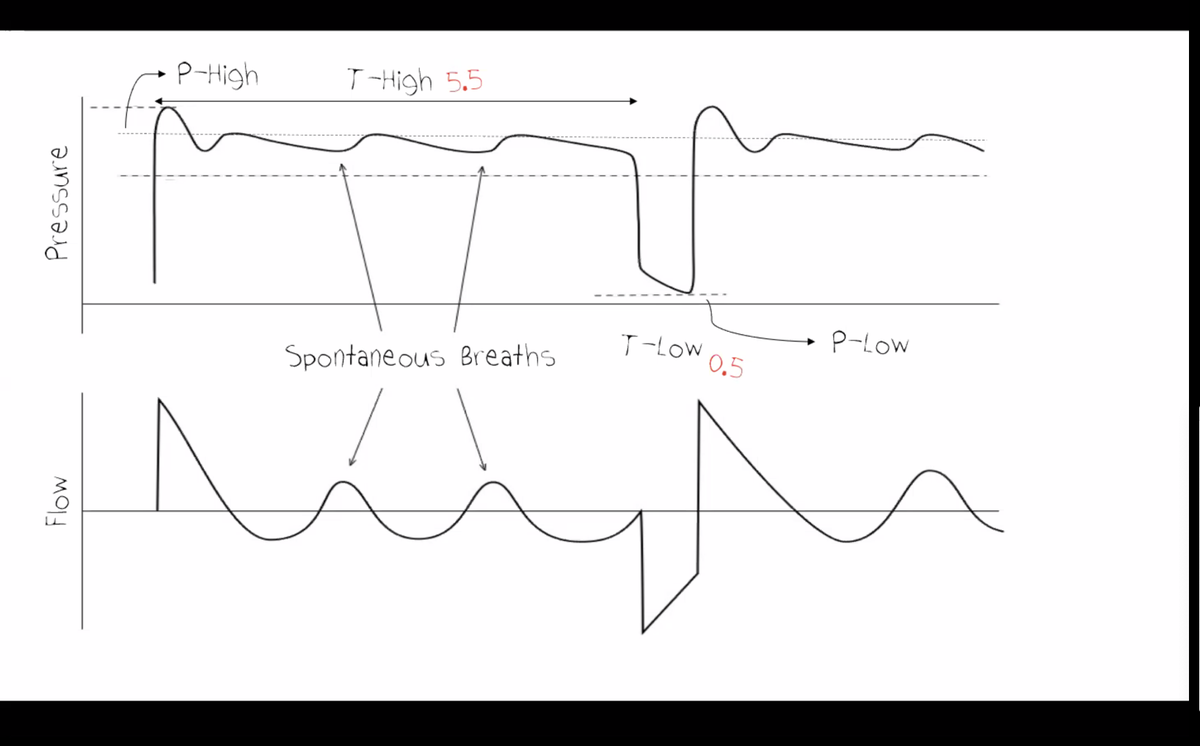
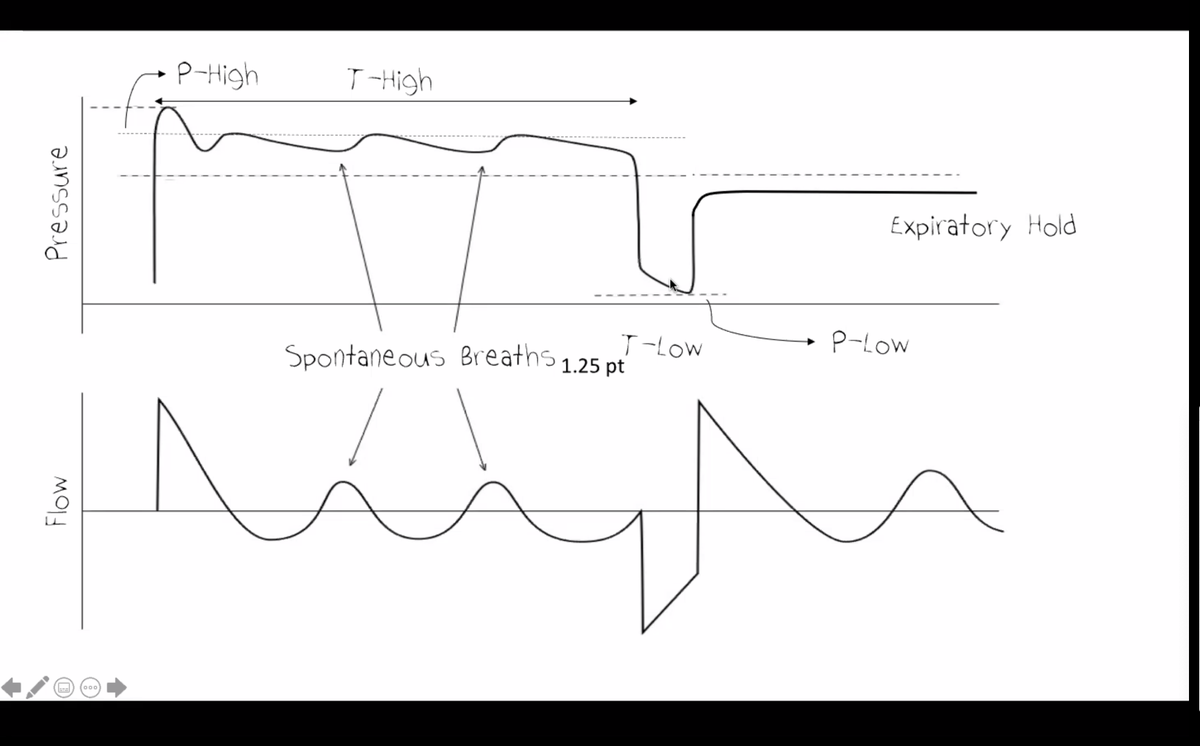
P-Hi: essentially the CPAP level, the pressure needed to achieve an adequate residual volume (FRC).
- @EMNerd_at #HRreloaded
- @EMNerd_at #HRreloaded
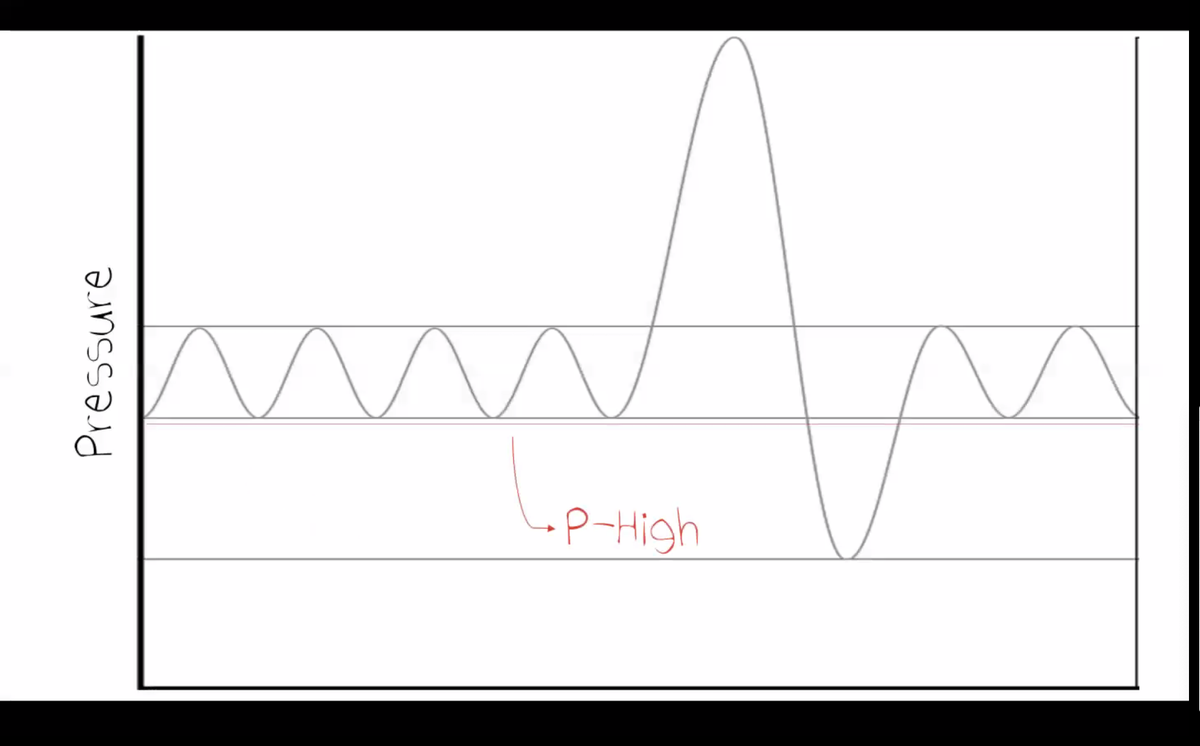
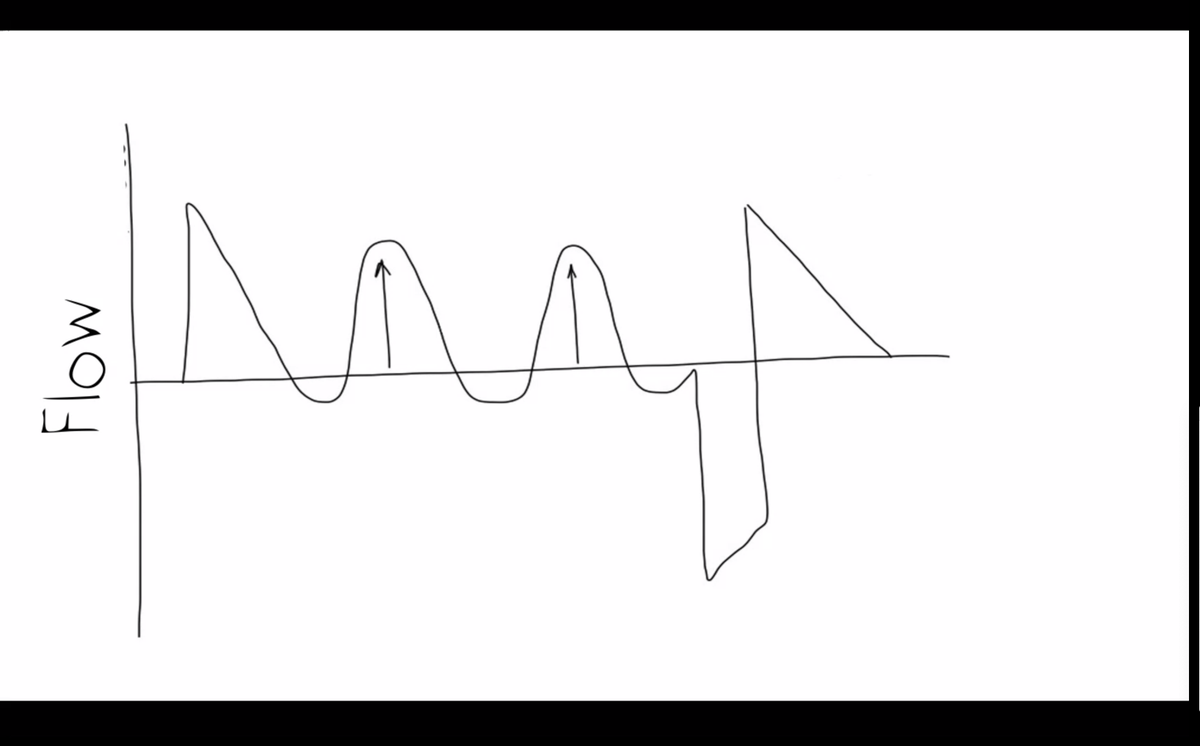
patient taking really huge breaths - may indicate that patient is under-distended and trying to re-inflate their lungs back to a normal FRC
- @EMNerd_at #HRreloaded
- @EMNerd_at #HRreloaded
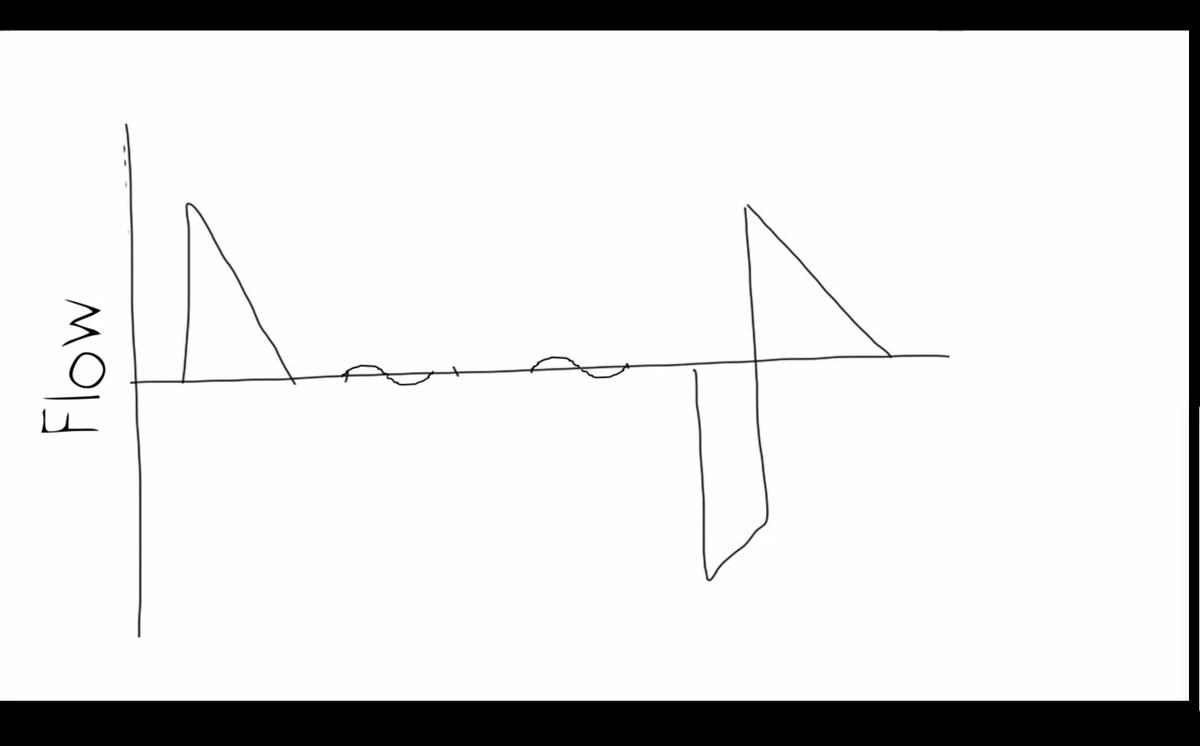
patient is unable to take adequate tidal volume - this may indicate the patient is over-inflated (and thus unable to further increase their lung volume)
- @EMNerd_at #HRreloaded
- @EMNerd_at #HRreloaded
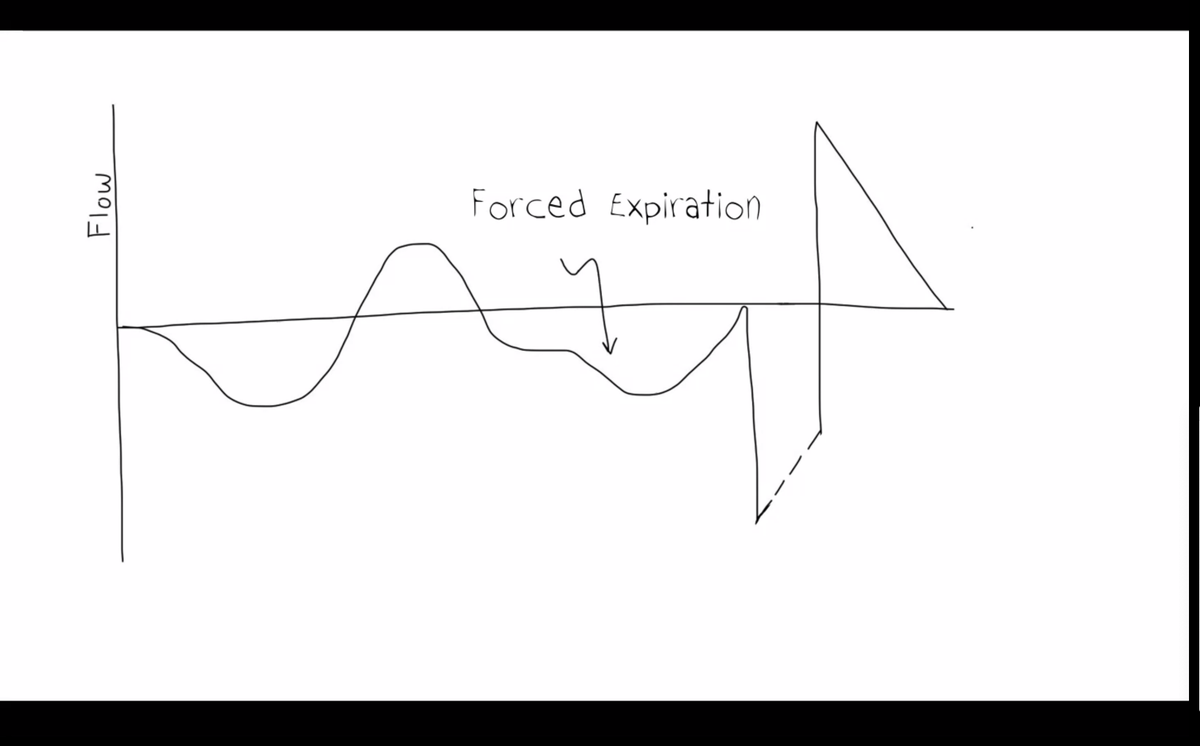
one sign that pHi is too high - patient is forcefully *exhaling* trying to reduce their lung volume back to normal.
- @EMNerd_at #HRreloaded
- @EMNerd_at #HRreloaded
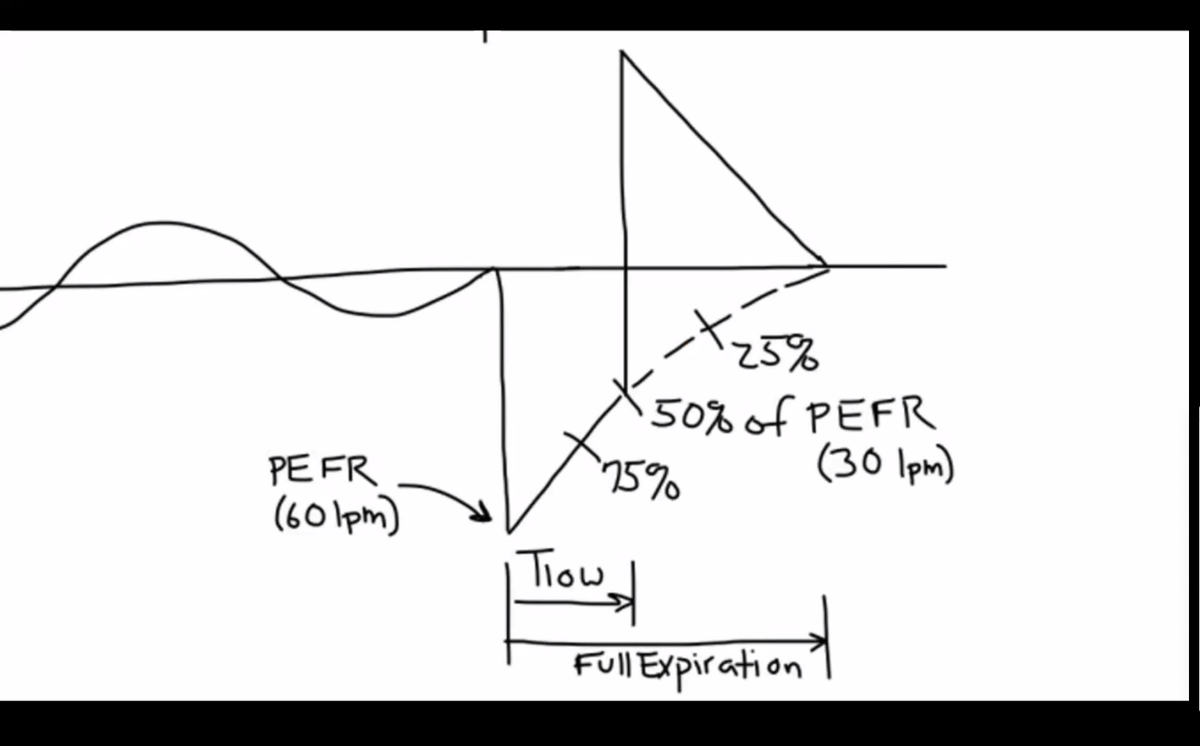
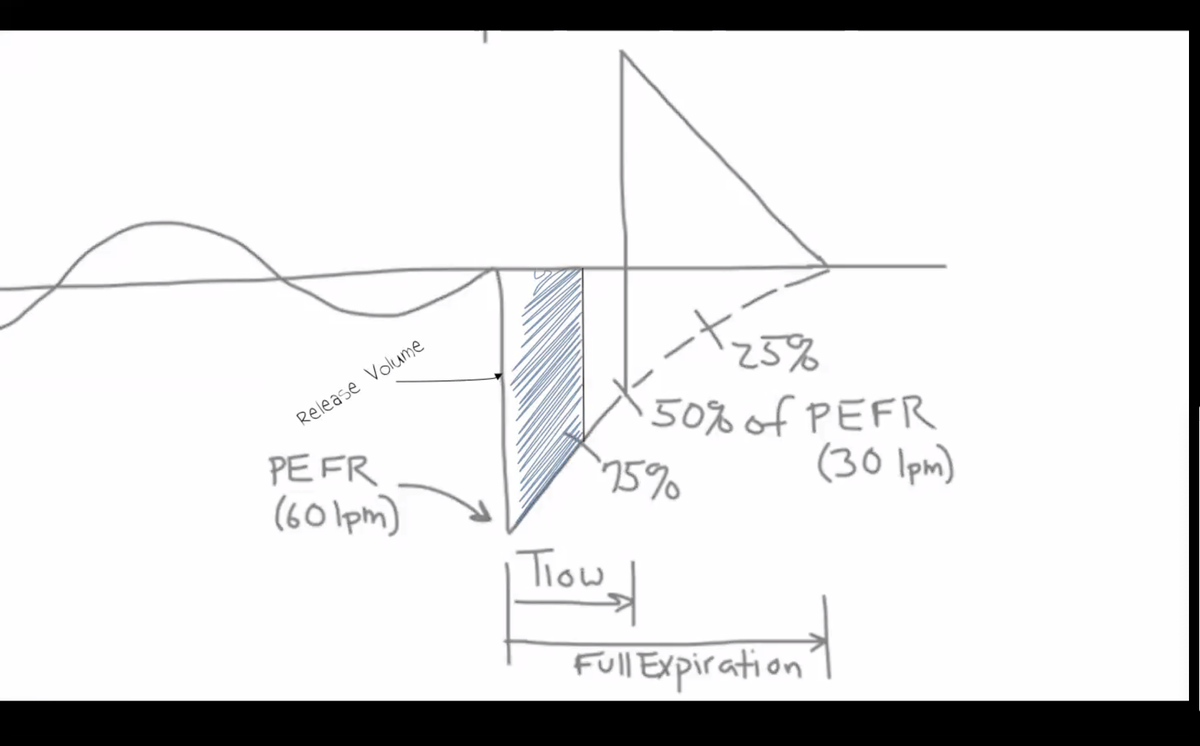
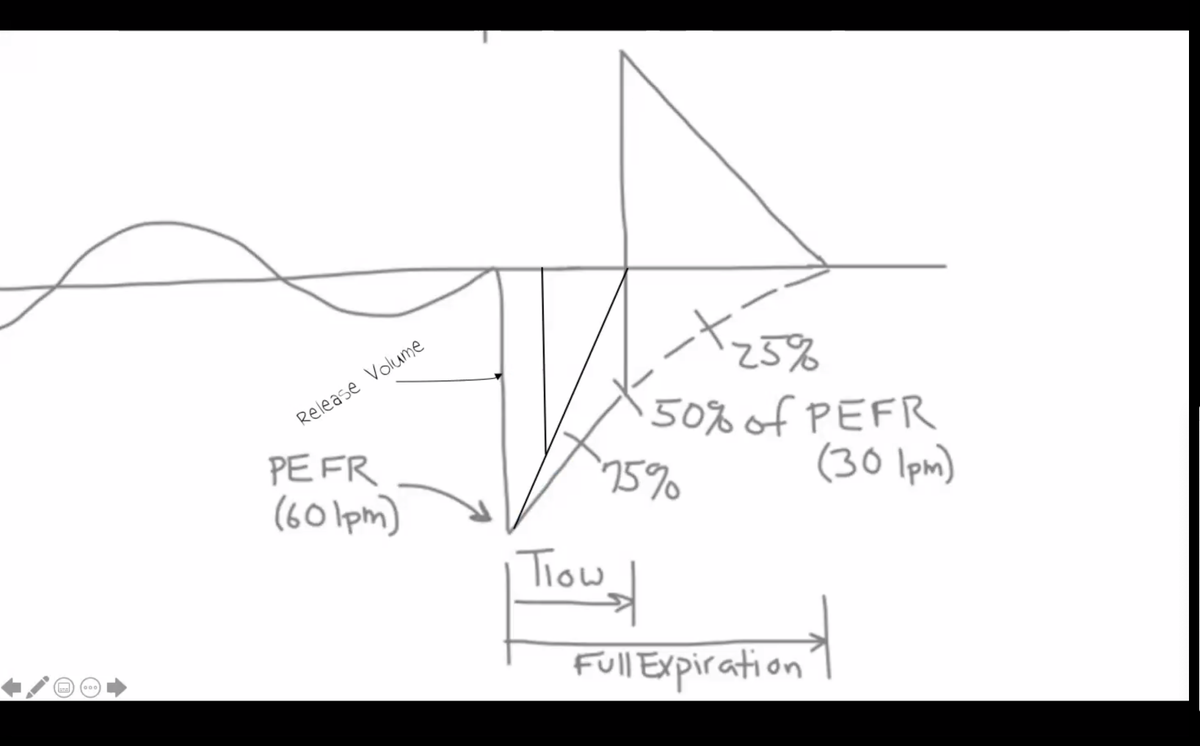
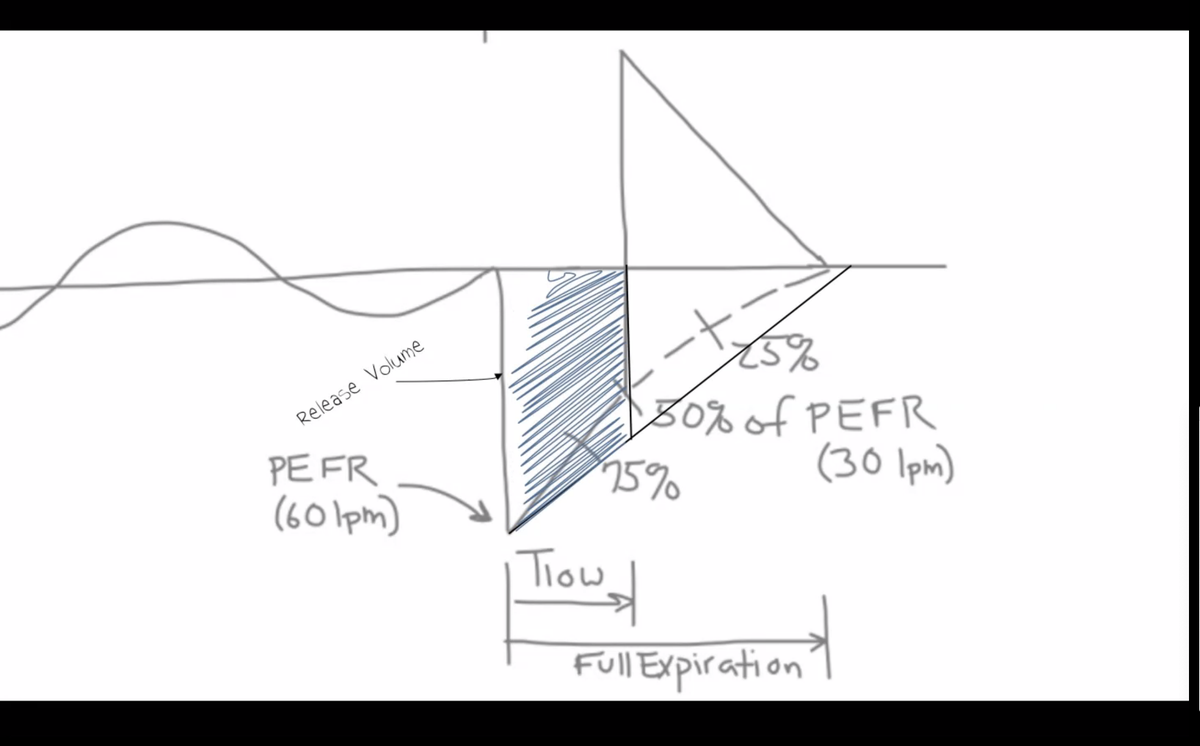
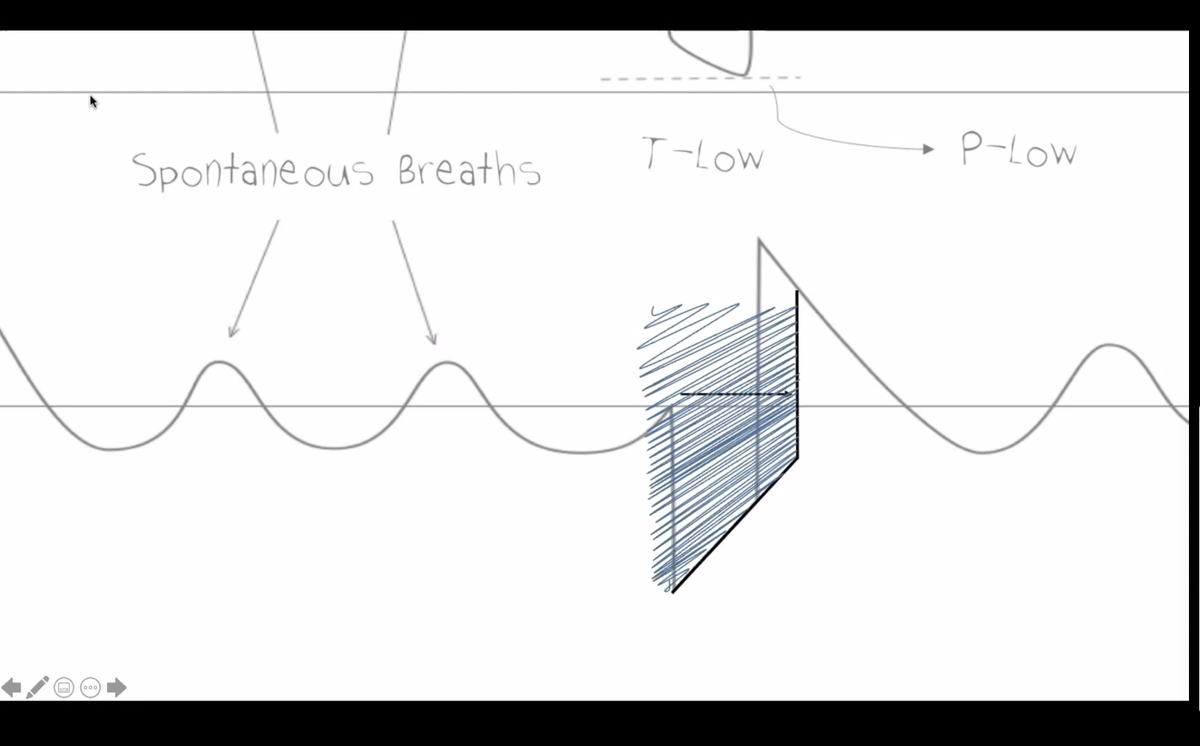
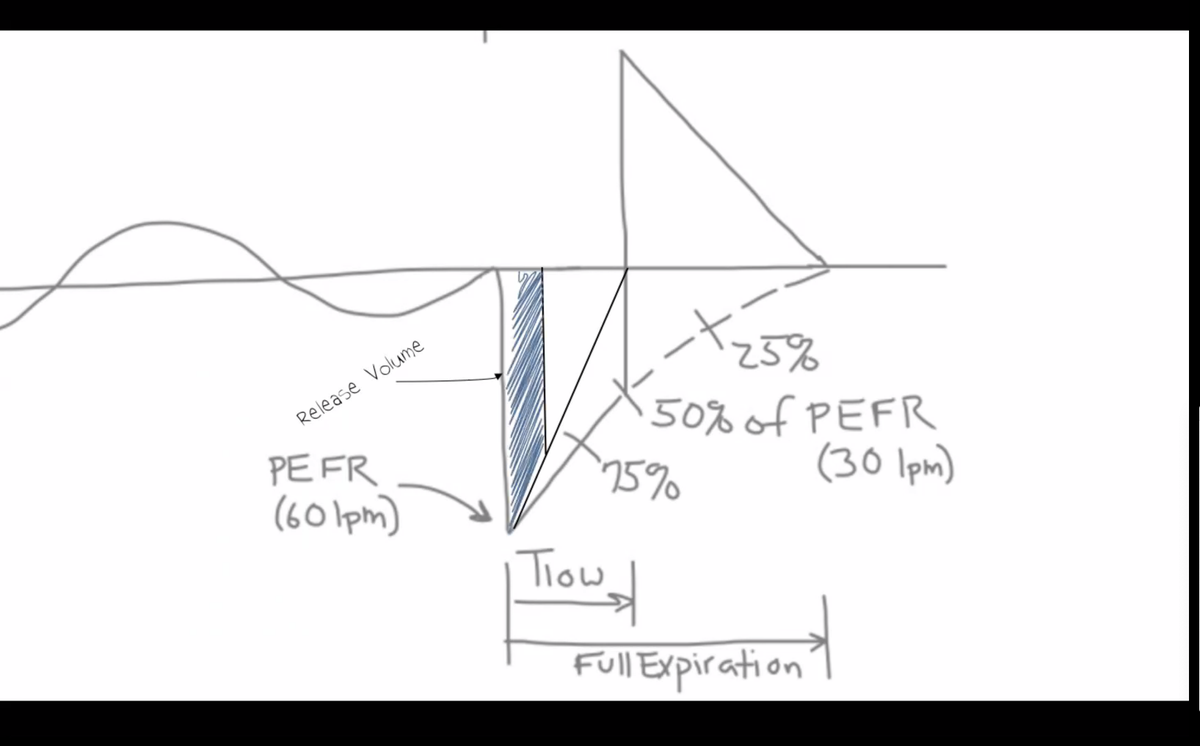
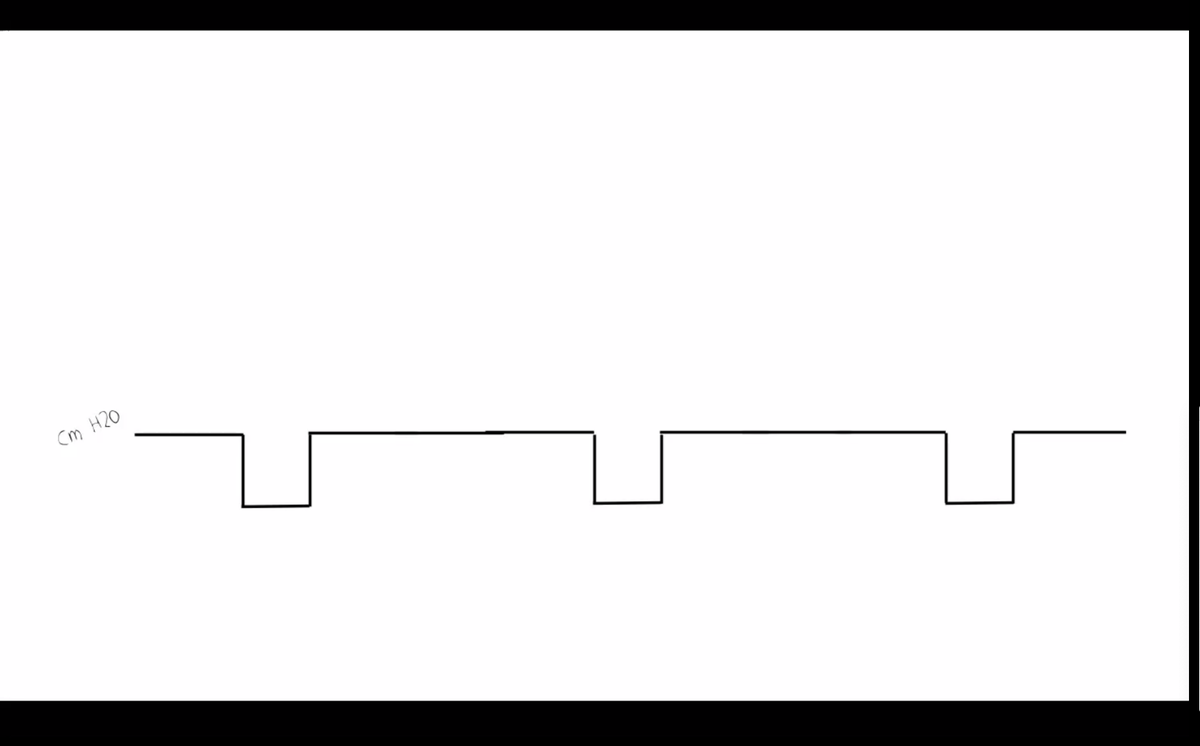
P-Low always set to zero - this makes things simple. The T-Low is used to control the effective PEEP (due to intentional gas trapping).
- @EMNerd_at #HRreloaded
- @EMNerd_at #HRreloaded
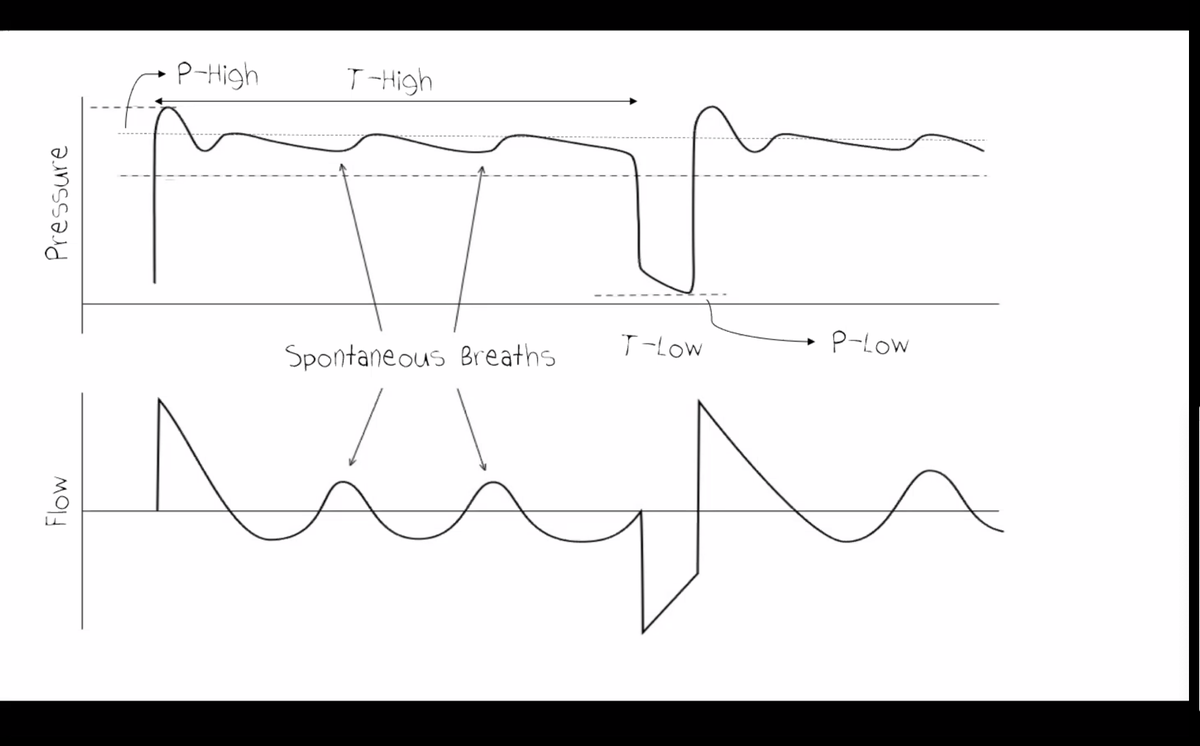
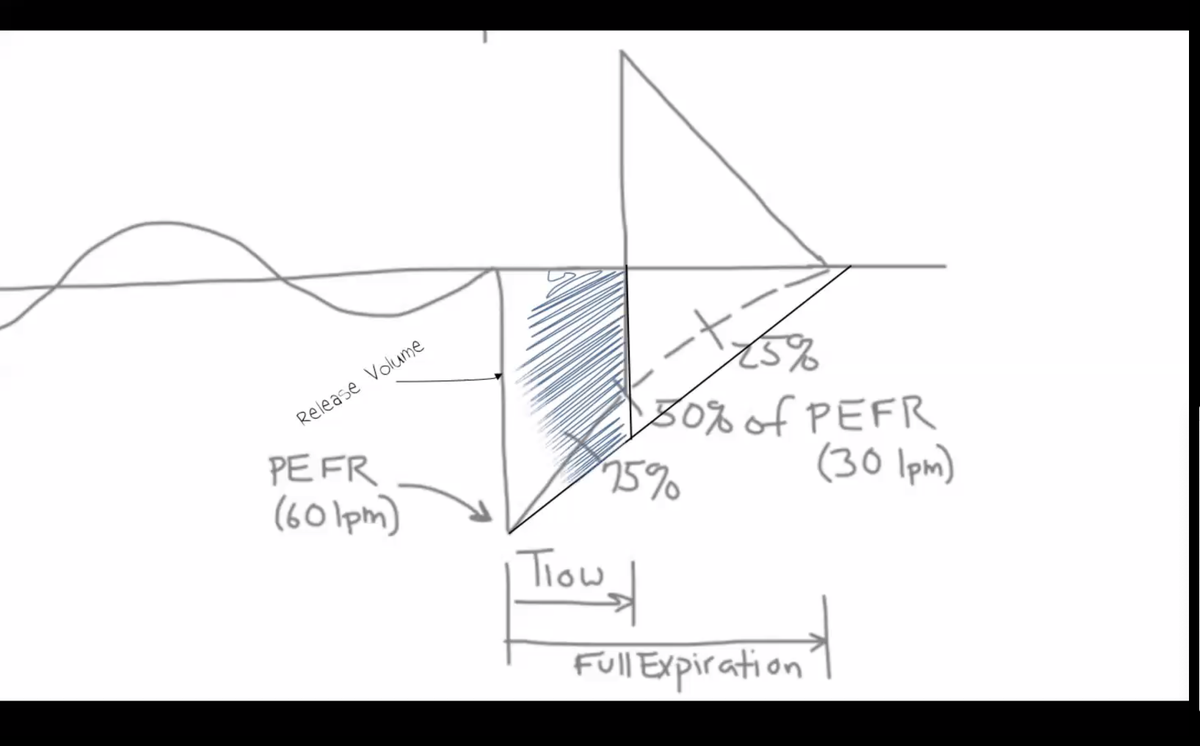
APRV uses time to control the expiatory volume. typically T-Low is used to truncate the flow at ~75% of the peak flow rate. this naturally reduces the tidal volume in the sickest patients!
- @EMNerd_at #HRreloaded
- @EMNerd_at #HRreloaded
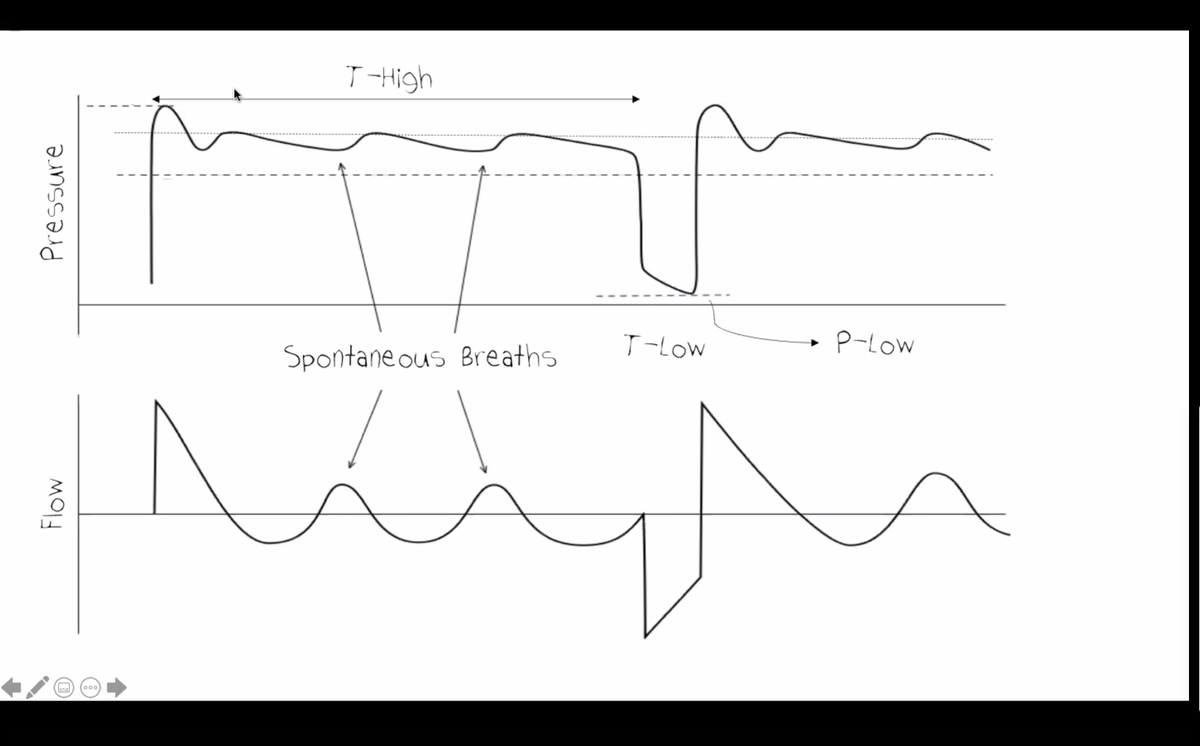
T-Hi improves recruitment and allows the patient to breathe spontaneously. However, higher T-Hi reduces the number of release volumes & bulk ventilation. often roughly start with Thi ~5.5, T-low ~0.5, PHi at plateau pressure -2 cm.
- @EMNerd_at #HRreloaded
- @EMNerd_at #HRreloaded
Drager is the Cadillac of APRV. some other vents may allow the patient to extend out their T-Low 😬
- @EMNerd_at #HRreloaded
- @EMNerd_at #HRreloaded

is spontaneous breathing dangerous? may be suggested by large excursion and poor clinical appearance on vent, in the initial phase of illness when the patient isn't ready to breathe much on their own. blunt resp drive with propofol and use dumping breaths to help clear CO2

what about ARDSnet? APRV naturally gives low TV in sickest patients with low compliance (~4 cc/kg). As lung compliance improves and patients improve, the tidal volume will naturally increase.
- @EMNerd_at #HRreloaded
- @EMNerd_at #HRreloaded

expiatory hold on APRV may be used to determine a driving pressure (pHi - expiratory pressure). If tidal volume is high but driving pressure is low, this may be reassuring.
- @EMNerd_at #HRreloaded
- @EMNerd_at #HRreloaded
what about hypercapnia? for any minute ventilation, APRV will achieve lower CO2 than conventional ventilation (due to diffusive CO2 clearance). lower T-Hi may provide more releases, which can improve CO2 clearance, but will impair recruitment.
- @EMNerd_at #HRreloaded
- @EMNerd_at #HRreloaded
To accelerate vent weaning, you *can* go directly to a spontaneous breathing trial from moderately high settings. So there isn't necessarily a single, rote approach to weaning - this can be personalized depending on how rapidly the patient is improving.
- @EMNerd_at #HRreloaded
- @EMNerd_at #HRreloaded
recruitment occurs over hours to days. studies describing recruitment over minutes may *fail* to detect recruitment in patients who might be able to recruit their lungs over a longer time period
- @EMNerd_at #HRreloaded
- @EMNerd_at #HRreloaded