

@GiJournal @AGA_Gastro @samirguptaGI @SultanMahmoodMD @8pm Before we move forward, lets define the polyps: #GIJC 
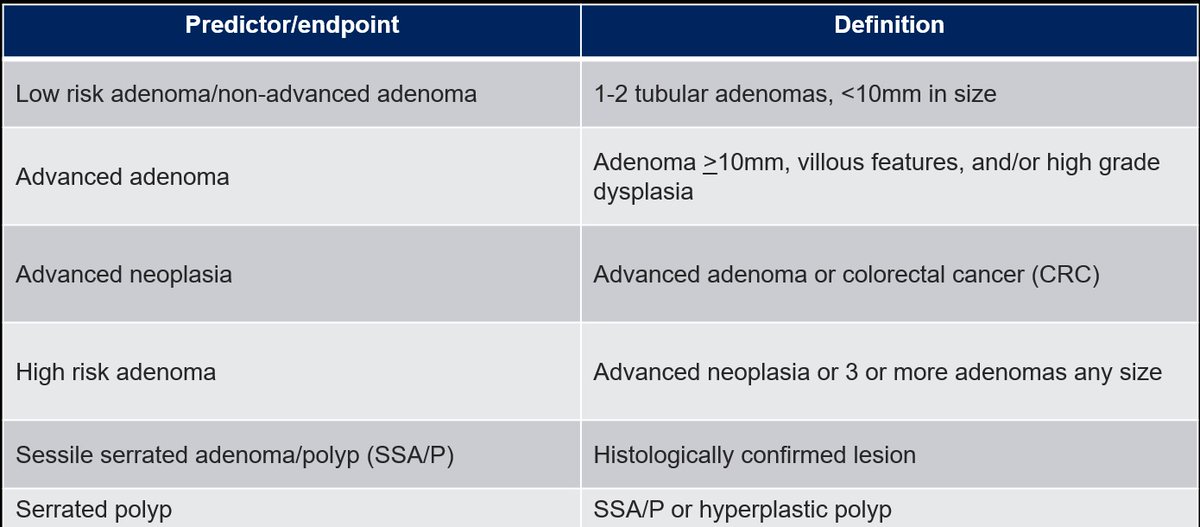
@GiJournal @AGA_Gastro @samirguptaGI @SultanMahmoodMD @8pm Post-polypectomy surveillance guidelines (for conventional adenomas/SPs) vary widely, and LOE is low. Therefore, the authors performed a prospective study (3 large cohort studies) to correlate the CRC risk with index screening precursors lesions. #GIJC
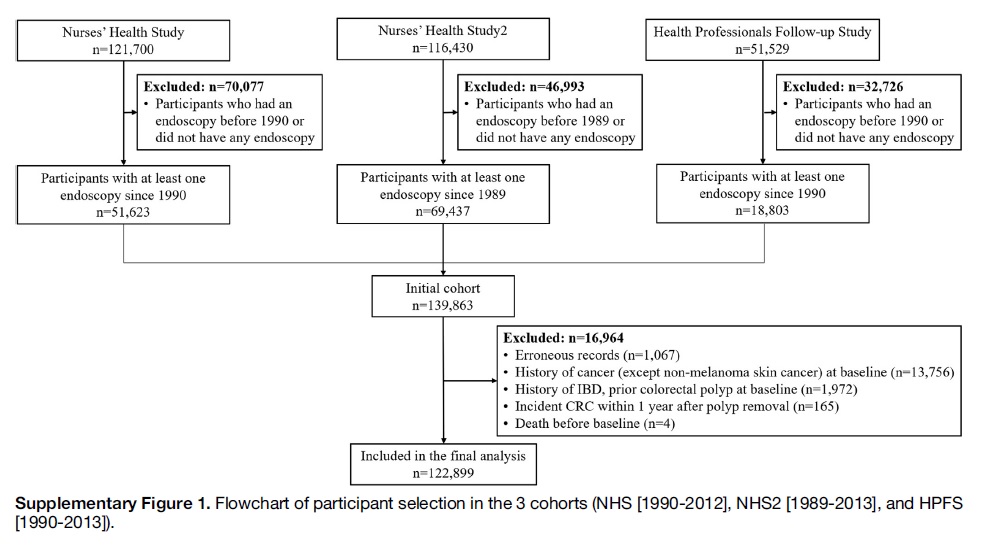
@GiJournal @AGA_Gastro @samirguptaGI @SultanMahmoodMD @8pm Methods: 3 large cohort studies (NHS, NHS2, HPFS) comprised a total of 122,899 patients. Avg follow-up rate >90% in all 3 cohorts via q2 years follow up.
Excluded; h/o CRC in last 1yr, prior polyp, IBD, previous endoscopy #GIJC
Excluded; h/o CRC in last 1yr, prior polyp, IBD, previous endoscopy #GIJC
@GiJournal @AGA_Gastro @samirguptaGI @SultanMahmoodMD @8pm Endo findings: No polyps, Conventional adenoma (adv vs non-adv), SPs (including HPs) Pts. followed q2 yrs. Risk factors assessed in covariate assessment. Accuracy of self-reported data 97-100%.
The cox-proportional hazard regression model used to cal. HRs for CRC incidence. #GIJC
The cox-proportional hazard regression model used to cal. HRs for CRC incidence. #GIJC
@GiJournal @AGA_Gastro @samirguptaGI @SultanMahmoodMD @8pm F/U 10 years. CRC incidence=491.
Conv adenoma: 51/6161, SP:24/5918, No polyps:427/112107.
Conv. adenoma group: 32% large lesion. 25% advanced histo. (19& TVA, 4% villous, 2% HGD)
SPs group:10% had at least 1 large SP, 10%>3 SPs #GIJC
Conv adenoma: 51/6161, SP:24/5918, No polyps:427/112107.
Conv. adenoma group: 32% large lesion. 25% advanced histo. (19& TVA, 4% villous, 2% HGD)
SPs group:10% had at least 1 large SP, 10%>3 SPs #GIJC
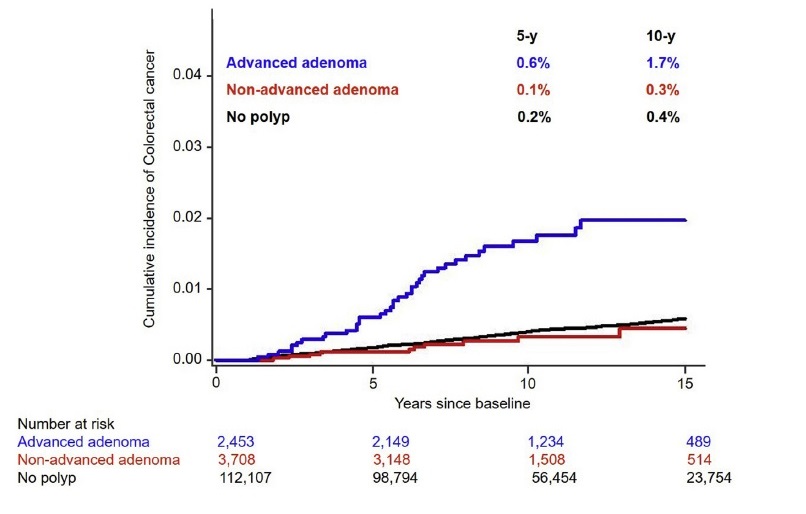
@GiJournal @AGA_Gastro @samirguptaGI @SultanMahmoodMD @8pm CRC cumulative incidence @ 5/10 median yr follow up:
-No polyp: 0.2%/ 0.4%
-Nonadv adneoma:0.1%/ 0.3%
-Adv. adenomas: 0.6%/ 1.7%
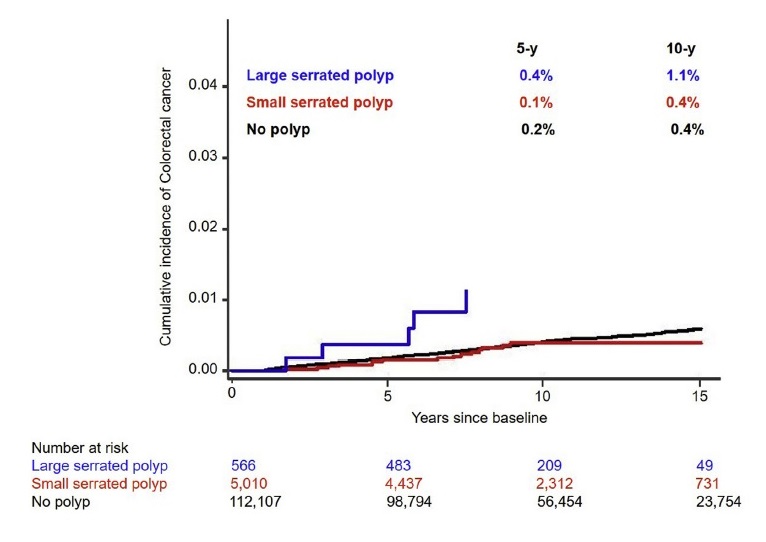
-Small SP: 0.1%/ 0.4%
-Large SPs: 0.4%/ 1.1% (all CRC cased dx within 6 yrs)
#GIJC
-No polyp: 0.2%/ 0.4%
-Nonadv adneoma:0.1%/ 0.3%
-Adv. adenomas: 0.6%/ 1.7%
-Small SP: 0.1%/ 0.4%
-Large SPs: 0.4%/ 1.1% (all CRC cased dx within 6 yrs)
#GIJC
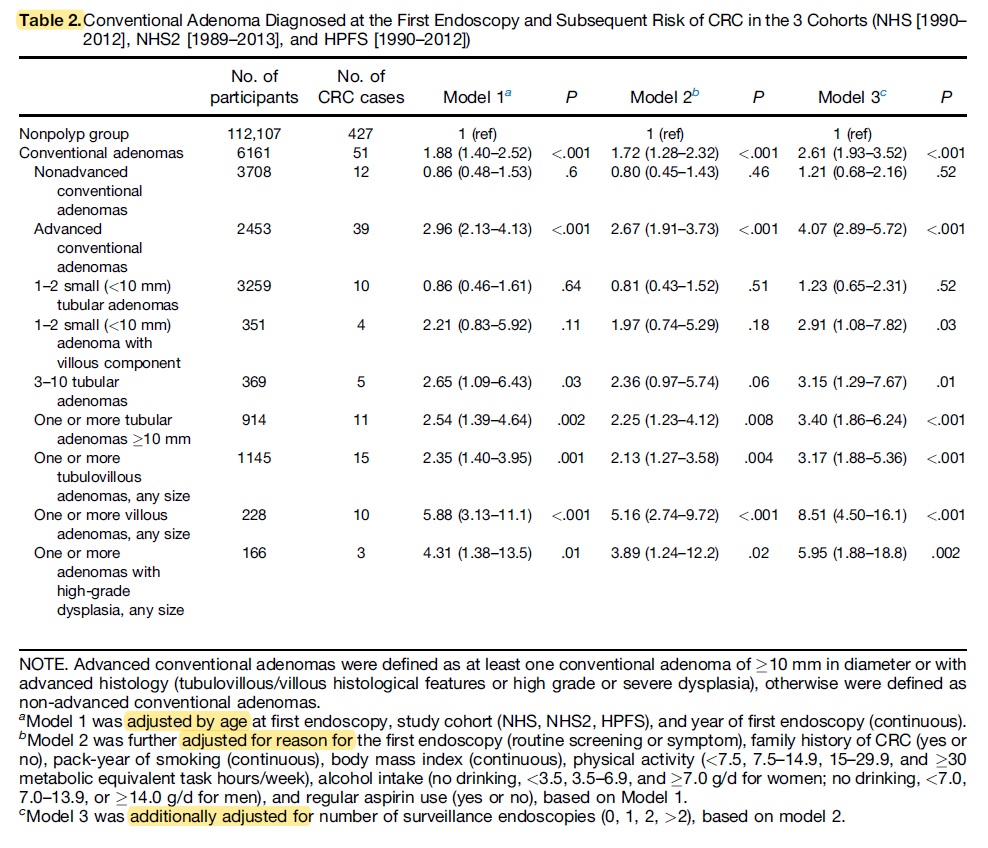
@GiJournal @AGA_Gastro @samirguptaGI @SultanMahmoodMD @8pm Diff. subtypes & CRC risk:
-Compared w/ no polyps, pts w/ advance adenomas had HR of 4.07. No association for non-adv adenoma
-HR for advanced histo: 3.17 for TVA, 8.51 for villous, 5.95 for HGD
-Size & # associated w/ high CRC risk. No risk elevation for 1-2 small adenoma
#GIJC
-Compared w/ no polyps, pts w/ advance adenomas had HR of 4.07. No association for non-adv adenoma
-HR for advanced histo: 3.17 for TVA, 8.51 for villous, 5.95 for HGD
-Size & # associated w/ high CRC risk. No risk elevation for 1-2 small adenoma
#GIJC
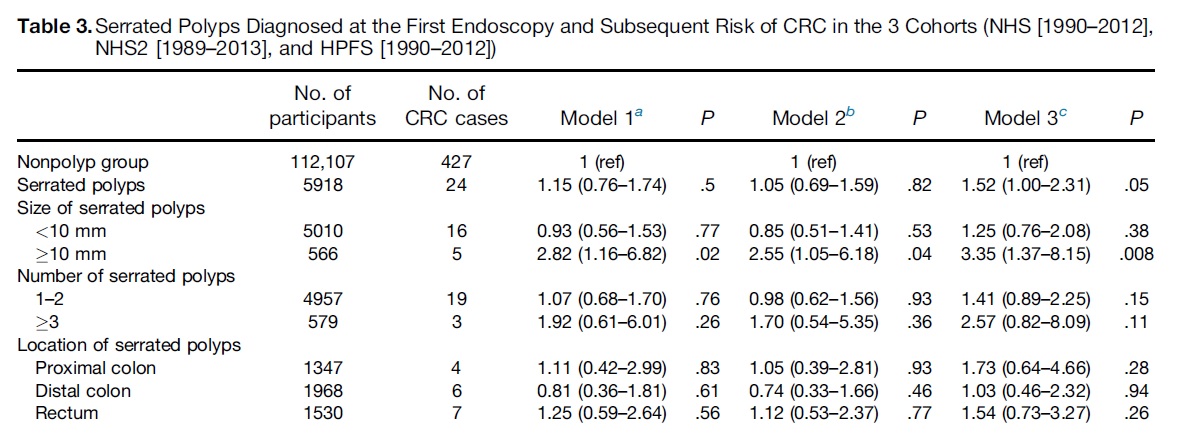
@GiJournal @AGA_Gastro @samirguptaGI @SultanMahmoodMD @8pm Similarly, SPs & CRC risk:
-Overall high risk. HR 1.52
-Larger SPs HR 3.35. Small SPs> No association.
-No association for # of polyps or sublocation.
> Compared to no polyp group, pts. w/ adenomas and SPs were at high CRC risk. HR 2.69 #GIJC
-Overall high risk. HR 1.52
-Larger SPs HR 3.35. Small SPs> No association.
-No association for # of polyps or sublocation.
> Compared to no polyp group, pts. w/ adenomas and SPs were at high CRC risk. HR 2.69 #GIJC
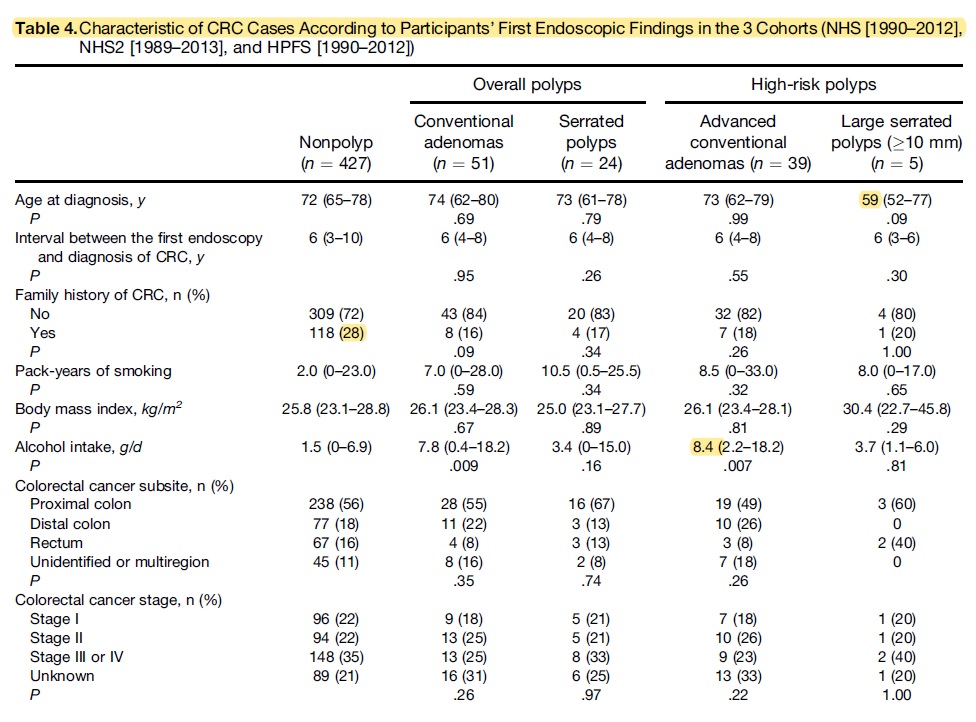
@GiJournal @AGA_Gastro @samirguptaGI @SultanMahmoodMD @8pm CRC characteristics:
Compared to other groups:
- Pts. w/ large SPs had CRC at a young age (median 59 years)
- CRC in nonpolyp group more likely to have fam history.
- CRC in conv. adenoma drank more alcoholics.
- No diff. in subsite, stage of CRC.
#GIJC
Compared to other groups:
- Pts. w/ large SPs had CRC at a young age (median 59 years)
- CRC in nonpolyp group more likely to have fam history.
- CRC in conv. adenoma drank more alcoholics.
- No diff. in subsite, stage of CRC.
#GIJC
@GiJournal @AGA_Gastro @samirguptaGI @SultanMahmoodMD @8pm Conclusion:
- 4x/3.35x increased CRC risk in advanced adenoma/large SPs> Justifies 3yr surveillance.
- No increased risk in non-adv adenomas or small SPs>
May not require intense surveillance than nonpolyp group
#GIJC
- 4x/3.35x increased CRC risk in advanced adenoma/large SPs> Justifies 3yr surveillance.
- No increased risk in non-adv adenomas or small SPs>
May not require intense surveillance than nonpolyp group
#GIJC
@GiJournal @AGA_Gastro @samirguptaGI @SultanMahmoodMD @8pm Strength: Long term f/u, polyp/CRC ascertainment, updated q2yrs patient data to avoid confounding
Limitations: unable to distinguish SPs from HPs. Surveillance data were self-reported> measurement error. No info on the quality of endoscopy. Some analyses based on small N.
#GIJC
Limitations: unable to distinguish SPs from HPs. Surveillance data were self-reported> measurement error. No info on the quality of endoscopy. Some analyses based on small N.
#GIJC

