
What 💊 provides ovarian cancer risk reduction, menstrual cycle regulation + symptom control, and pregnancy prevention? Oral contraception a.k.a. “birth control pills.”
Intimidated by prescribing hormones? Here's what you need to know to prescribe safely and effectively.
Intimidated by prescribing hormones? Here's what you need to know to prescribe safely and effectively.
First, make sure that an OCP is appropriate for your patient. My favorite source is the CDC Medical Eligibility Criteria:
cdc.gov/reproductivehe…
cdc.gov/reproductivehe…

Which two hormones are in Oral Contraceptive Pills (OCPs)?
You got it! Combined hormonal contraceptive pills = an estrogen + a progestin.
The most common estrogen used is ethinyl estradiol (EE). There are 4 gen of progestins.
The (a) type of progestin and (b) amount of each component are what make each OCP unique.
The most common estrogen used is ethinyl estradiol (EE). There are 4 gen of progestins.
The (a) type of progestin and (b) amount of each component are what make each OCP unique.
Pills are presented as a name (brand or generic) followed by the amount of each component. E.g.: Estarylla (EE 0.035 mg / norgestimate 0.25mg).
The progestin component is dominant. Its job is to suppress the LH surge, thereby preventing ovulation. It also thickens cervical mucus, thins the endometrium, and decreases Fallopian tubal motility. You can generally go with a lower dose (e.g., 0.4mg norethindrone).
EE suppresses FSH (to prevent emergence of a dominant follicle) and stabilizes the endometrium. EE comes in 20mcg or 35mcg doses. 35mcg pills are more common, with “low-dose” 20mcg pills typically prescribed for obese patients or women >40yo. (For these pts consider a POP.)
OCP pill packs have 21 active (EE + progestin) & 7 placebo pills. You can vary the amount of EE and progestin in each week of the active pills in order to mimic physiologic hormone cycling.
Pill pack:
💊💊💊💊💊💊💊
💊💊💊💊💊💊💊
💊💊💊💊💊💊💊
✖️✖️✖️✖️✖️✖️✖️
Pill pack:
💊💊💊💊💊💊💊
💊💊💊💊💊💊💊
💊💊💊💊💊💊💊
✖️✖️✖️✖️✖️✖️✖️
Different oral formulations:
- Monophasic = same amt EE & progestin in each pill. These are the most common!
- Estrogenic = consistent EE dose + varying progestin dose as the pill pack progresses.
- Multiphasic = a varying amount of EE and progestin each week
- Monophasic = same amt EE & progestin in each pill. These are the most common!
- Estrogenic = consistent EE dose + varying progestin dose as the pill pack progresses.
- Multiphasic = a varying amount of EE and progestin each week
The next question is how often the patient wants a withdrawal bleed. If she wants to have a monthly bleed, prescribe 21 (3wk) active pills ➡️ 7 (1wk) placebo pills. If she wants to bleed less often than monthly, that’s called “extended dosing.” Tell her to skip the placebo pills.
There is no physical benefit to having a monthly bleed. Some women like the monthly bleed as reassurance of lack of pregnancy. It’s solely about patient preference.
Almost there! The patient is ready to start taking her Rx. There are 3 ways to start: immediately, Sunday, or day 1 of menses. If you choose any other method than day 1, backup contraception is recommended for 7 days. Doesn’t really matter which you choose.
Hold up, it's that easy? Yes indeed. Now let's prepare you for the troubleshooting you may need to do.
Common problem #1: BREAKTHRU BLEEDING. Inconvenient, but does not indicate ⬇️ contraceptive efficacy! Typically due to excess thinning of the endometrium from the progestin to the point where there are small denuded spots with exposed, friable blood vessels.
Options to tx BTB:
- Stop the active pills x1wk, allow a withdrawal bleed, then restart.
- Prescribe extra estrogen (e.g., Premarin 1.25mg x7d). If that doesn’t work, you can repeat once.
If your fix fails, look for a structural cause of the bleeding (eg, endometrial polyp).
- Stop the active pills x1wk, allow a withdrawal bleed, then restart.
- Prescribe extra estrogen (e.g., Premarin 1.25mg x7d). If that doesn’t work, you can repeat once.
If your fix fails, look for a structural cause of the bleeding (eg, endometrial polyp).
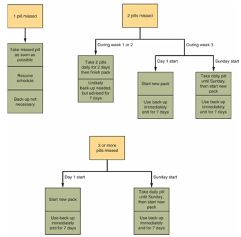
Common problem #2: Missed doses. Follow this handy dandy chart from Speroff (THE reproductive endocrinology and infertility textbook):
Common problem #3: Your patient is about to enter the phase of her life where she desires pregnancy. When do you tell her to stop taking the pills?
We recommend stopping pills 2mo prior to desired pregnancy in order to improve the accuracy of pregnancy dating (by providing a more reliable Last Menstrual Period). As an FYI, taking OCPs at current day doses does not affect future fertility!
In sum, to prescribe OCPs easily & safely:
💊 Make sure OCPs are safe for your patient.
💊Pick a progestin.
💊Pick EE & progestin doses
💊Find out how often a withdrawal bleed is desired.
💊Choose when to start the pills.
💊Troubleshoot problems
💊 Stop 2mo prior to desired preg
💊 Make sure OCPs are safe for your patient.
💊Pick a progestin.
💊Pick EE & progestin doses
💊Find out how often a withdrawal bleed is desired.
💊Choose when to start the pills.
💊Troubleshoot problems
💊 Stop 2mo prior to desired preg
📚 References 📚
🌟 Inspired by Dr. Michael Thomure (St Louis University REI) ⚜️
🌟 Speroff’s Clinical Gynecologic Endocrinology & Infertility
🌟 C.D.C. Medical Eligibility Criteria
🌟 Inspired by Dr. Michael Thomure (St Louis University REI) ⚜️
🌟 Speroff’s Clinical Gynecologic Endocrinology & Infertility
🌟 C.D.C. Medical Eligibility Criteria

