
As we think about convalescent plasma (CP), I thought it was worth looking at the actual data in other diseases. As best I can tell, the only actual trial showing efficacy for CP is in Argentine hemorrhagic fever, published in Lancet in 1979. It's an elegant study from 1974–1978

They blinded (using FFP as the control) and enrolled based on high clinical suspicion. Among the 217 enrolled, 188 had confirmed AHF. The money shot is this one: (p=0.0002 by Fisher's exact). 
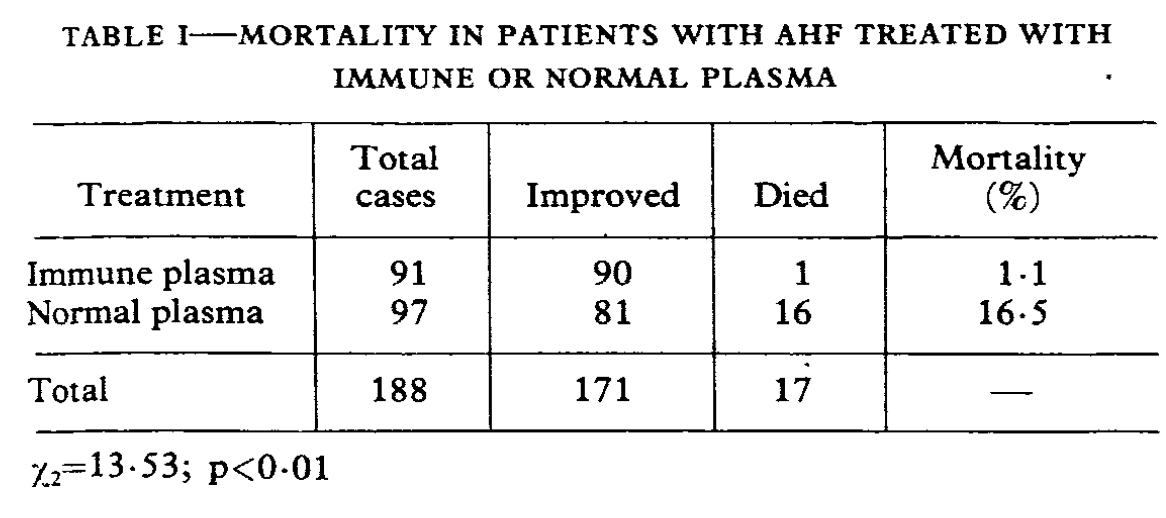
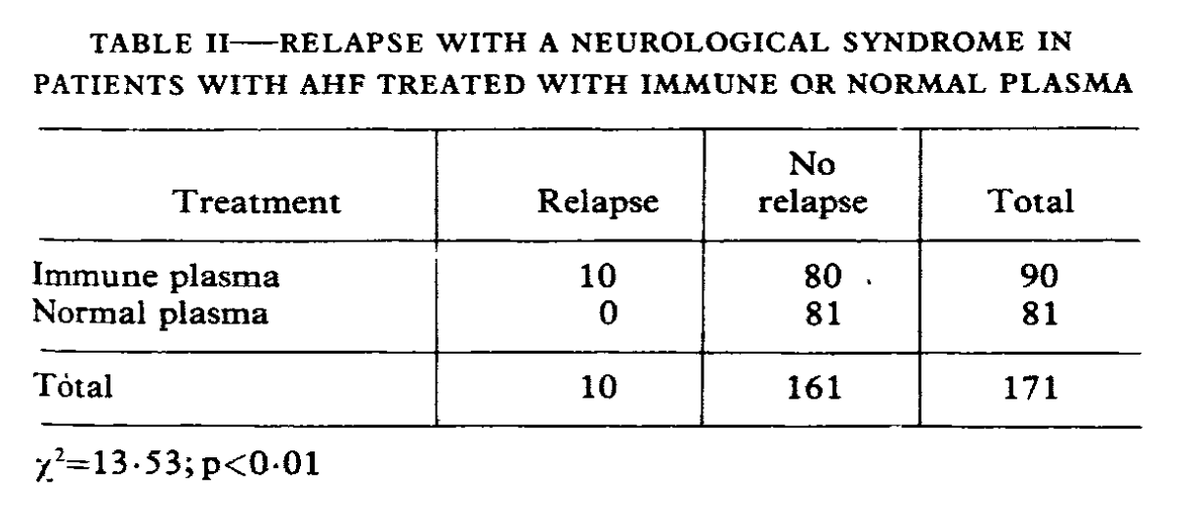
Nice. Turns out you really can do RCTs of convalescent plasma. But that's not the whole story--it turns out that there's a relapsing neurological syndrome that is dramatically more common in patients treated with CP. The one death in the CP arm actually happened as a result of
the neurological syndrome.
My take home--do the RCTs, and carefully watch for late safety signals. The more I read the more convinced I am that CP belongs in trials, not in ubiquitous clinical use.
• • •
Missing some Tweet in this thread? You can try to
force a refresh



