
A new Tweetorial from @LorinskyMD!
After taking a deep dive into AKI management last week, I was left wondering, what is the deal with the FENa?
After taking a deep dive into AKI management last week, I was left wondering, what is the deal with the FENa?
Despite urine lytes being sent often, I haven’t found it very useful clinically.
But what does the evidence show?
But what does the evidence show?
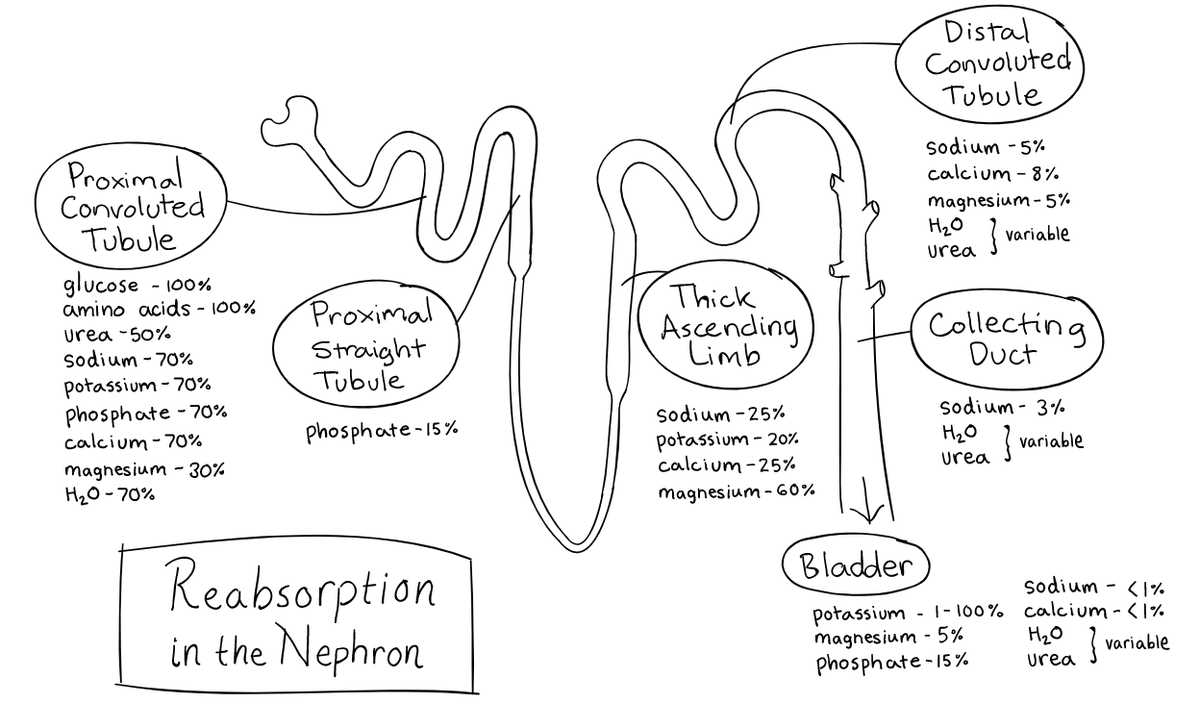
FENa is fractional excretion of sodium. Classically, the idea is with hypovolemic prerenal states, the kidney is sodium avid, and FENa is < 1% 

But if the patient develops ATN, then FENa is >3%, because the tubules can’t resorb sodium properly. Great! Should help me differentiate prerenal AKI from ATN
(h/t @khanacademy for the great image)
(h/t @khanacademy for the great image)
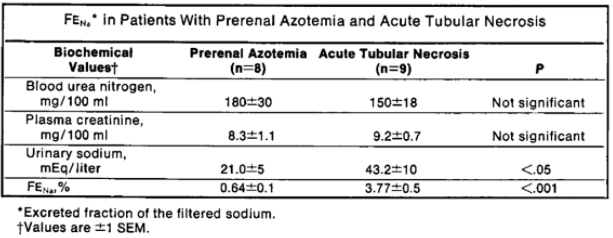
How did this thinking come to be? A JAMA 1976 paper studied only 17 cases of AKI in the *oliguric phase*, they found that the FENa was able to differentiate prerenal/ATN with p value of < 0.001
source: pubmed.ncbi.nlm.nih.gov/947239/
source: pubmed.ncbi.nlm.nih.gov/947239/
Additional prospective studies, like this one from Diskin et al. in 2010, confirmed the utility of FENa (and FEUrea) as helpful diagnostically for prerenal vs tubular injury
source: europepmc.org/article/med/19…
source: europepmc.org/article/med/19…
So why haven’t I found it as helpful in clinical practice?
The FENa was also the star of a 2016 @JHospMedicine @TWDFNR piece by @Pahwa and @JohnSperati.
So where does the FENa fail?
source: journalofhospitalmedicine.com/jhospmed/artic…
So where does the FENa fail?
source: journalofhospitalmedicine.com/jhospmed/artic…
First, FENa was validated for patients specifically with *oliguric AKI* (< 20 mL/hr in the paper).
Lots of things can also through FENa off, including:
1️⃣ Older age
2️⃣ Baseline CKD
3️⃣ Diuretic use
Lots of things can also through FENa off, including:
1️⃣ Older age
2️⃣ Baseline CKD
3️⃣ Diuretic use
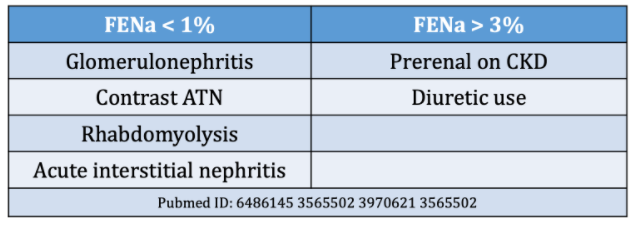
That is to say, FENa can be nonspecific -- low in other non-prerenal states, and high in non-ATN states.
What are potential confounders?
What are potential confounders?
When @JHospMedicine calculated the likelihood ratios based on Diskin et al.’s 2010 prospective study of 100 pts with oliguric AKI, they found a LR of 1.1-3.8 for FENa (and better for FEUrea).

Urine lytes are cheap to order, and appear to be modestly predictive (better with FeUrea) between pre-renal and ATN. But is FENa still worth the effort to calculate? Especially if it may confound the diagnosis?
Is it a Thing We Do For No Reason? The answer is maybe!
In an oliguric patient with no renal dysfunction at baseline, FENa can help to differentiate prerenal disease and ATN, as long as you keep in mind the confounding situations.
In an oliguric patient with no renal dysfunction at baseline, FENa can help to differentiate prerenal disease and ATN, as long as you keep in mind the confounding situations.
But with so many caveats, my **personal opinion** is it shouldn’t be sent if you have any clinical suspicion at all for prerenal disease, for which fluid challenge is both diagnostic/therapeutic.
If you want to read more, @medrants also broke this down. Welcome any more thoughts and tips of FENa in practice

