
2020 ESC Guidelines on NSTEACS:
- 10 key concepts to remember and messages that will change our practice -
#ESCCongress #ESC_Acute #Acutecvd
- 10 key concepts to remember and messages that will change our practice -
#ESCCongress #ESC_Acute #Acutecvd
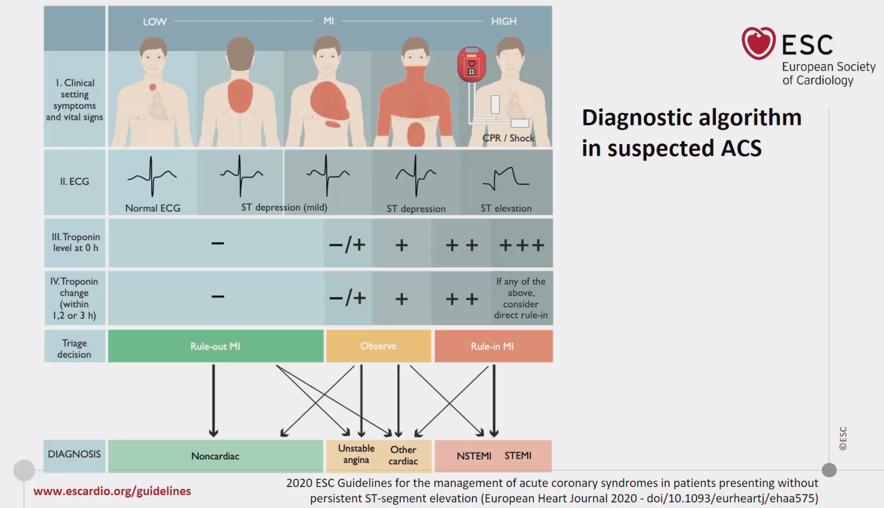
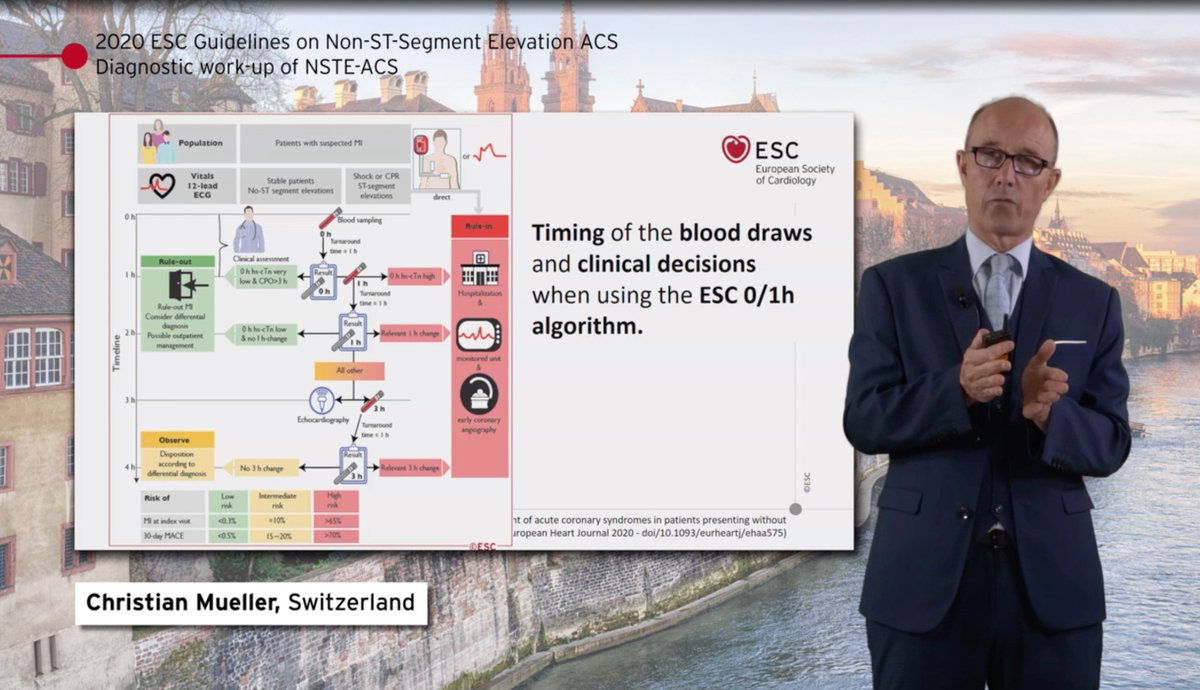
1/ Diagnosis of NSTEACS is based on
- Symptoms
- EKG
- Initial c-TnI concentrations
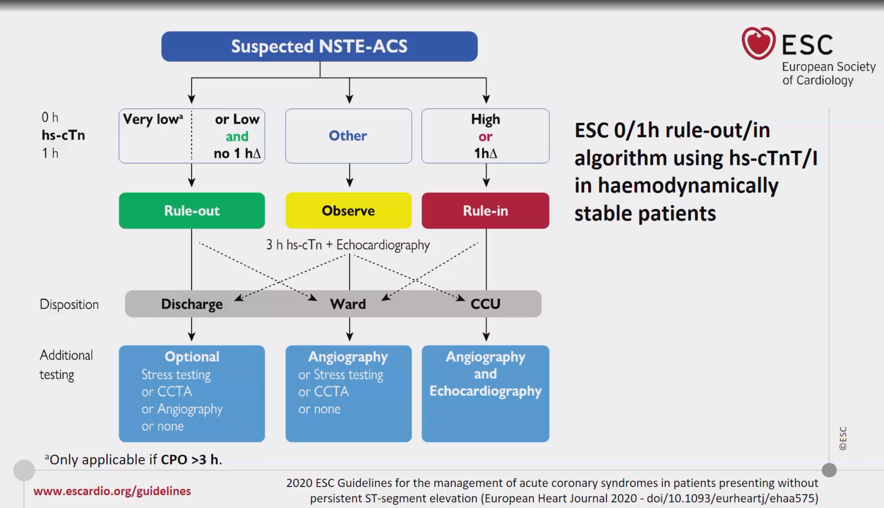
- Subsequent c-TnI (0-1; 0-2; 0-3h if hs-cTn)
- Symptoms
- EKG
- Initial c-TnI concentrations
- Subsequent c-TnI (0-1; 0-2; 0-3h if hs-cTn)
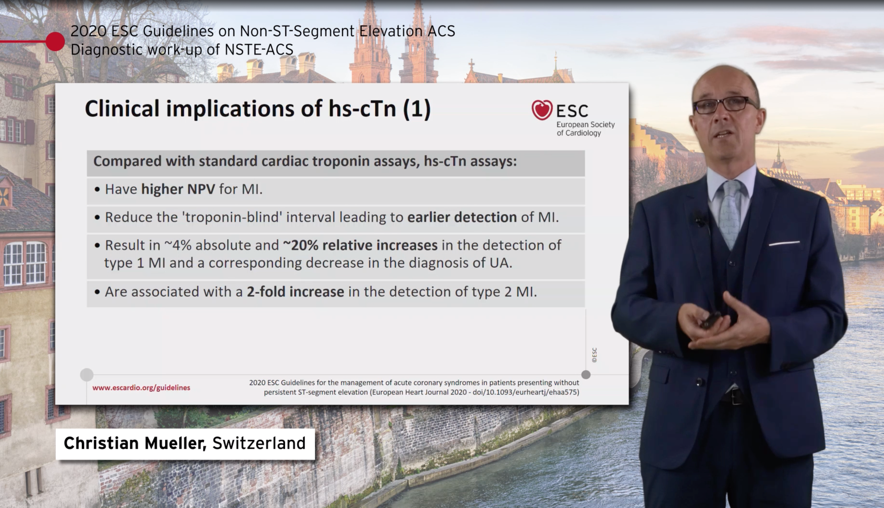
2/ To remember:
Hs cardiac troponin is a myocardial injury biomarker: not only MI biomarker!
Concentrations >99th percentile may respond to different diagnoses. Clinical presentation / context must be taken into account.
Timing of blood draw is important to choose cutoffs
Hs cardiac troponin is a myocardial injury biomarker: not only MI biomarker!
Concentrations >99th percentile may respond to different diagnoses. Clinical presentation / context must be taken into account.
Timing of blood draw is important to choose cutoffs
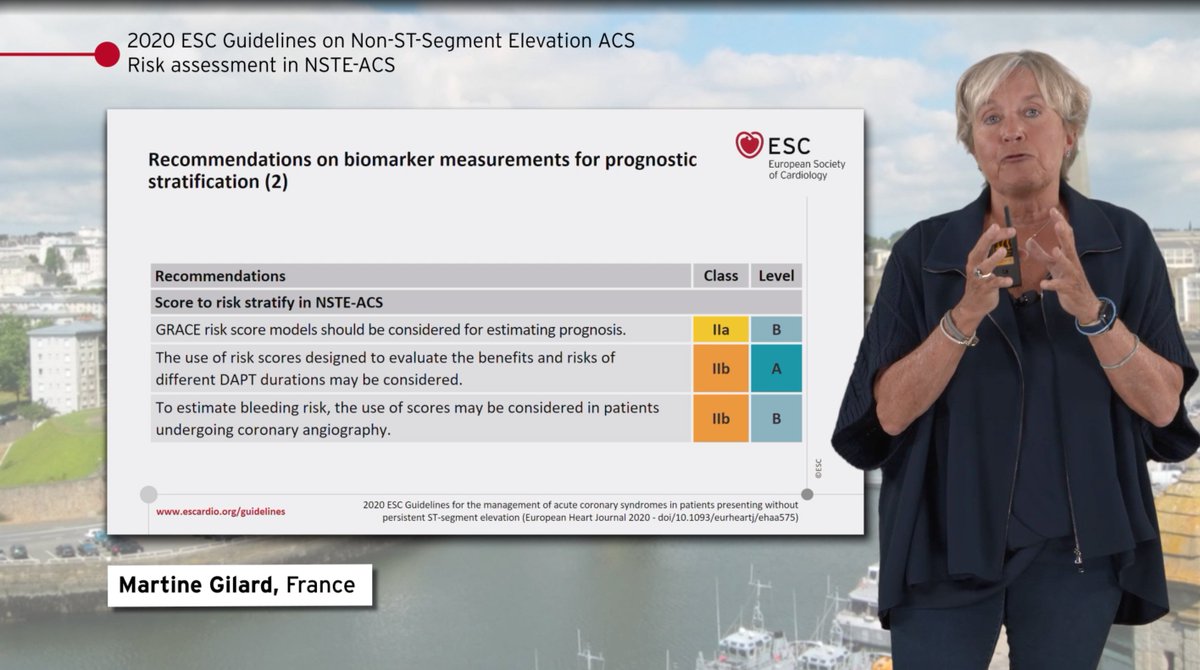
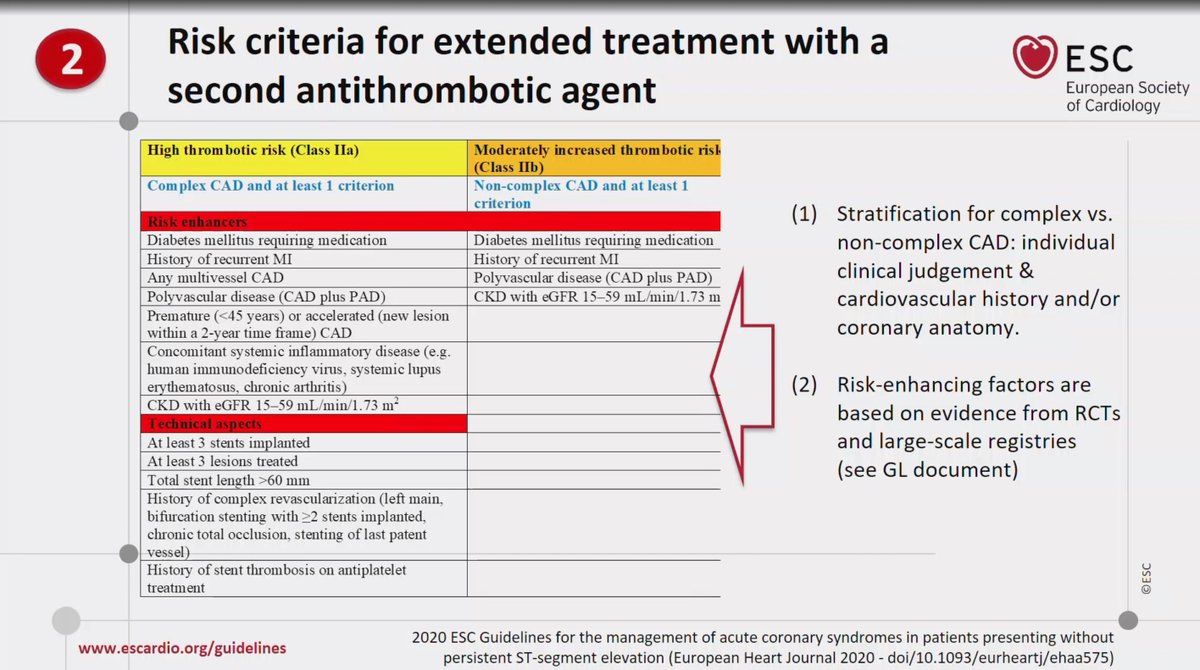
3/ Risk stratification
EKG: ST segment depression>T wave inv
Biomarkers: natriuretic peptides, hs-cTn
Risk scores: GRACE
Bleeding scores: ARC-HRB; needs validation!
- Integrate with DAPT, PRECISE DAPT
EKG: ST segment depression>T wave inv
Biomarkers: natriuretic peptides, hs-cTn
Risk scores: GRACE
Bleeding scores: ARC-HRB; needs validation!
- Integrate with DAPT, PRECISE DAPT


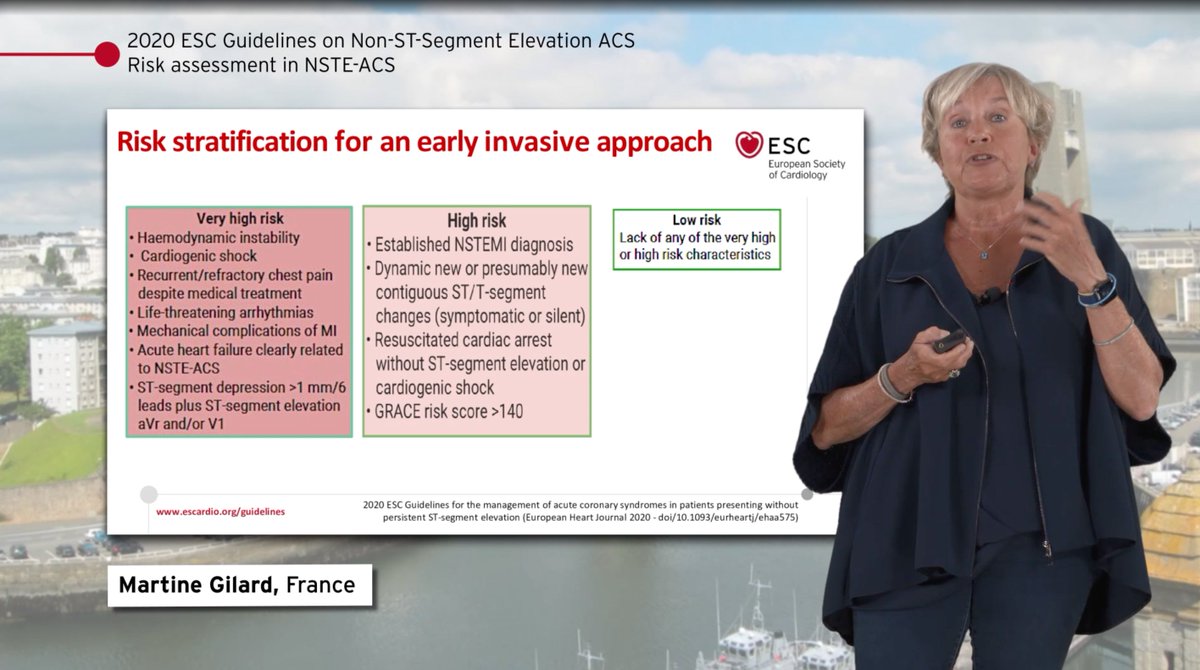
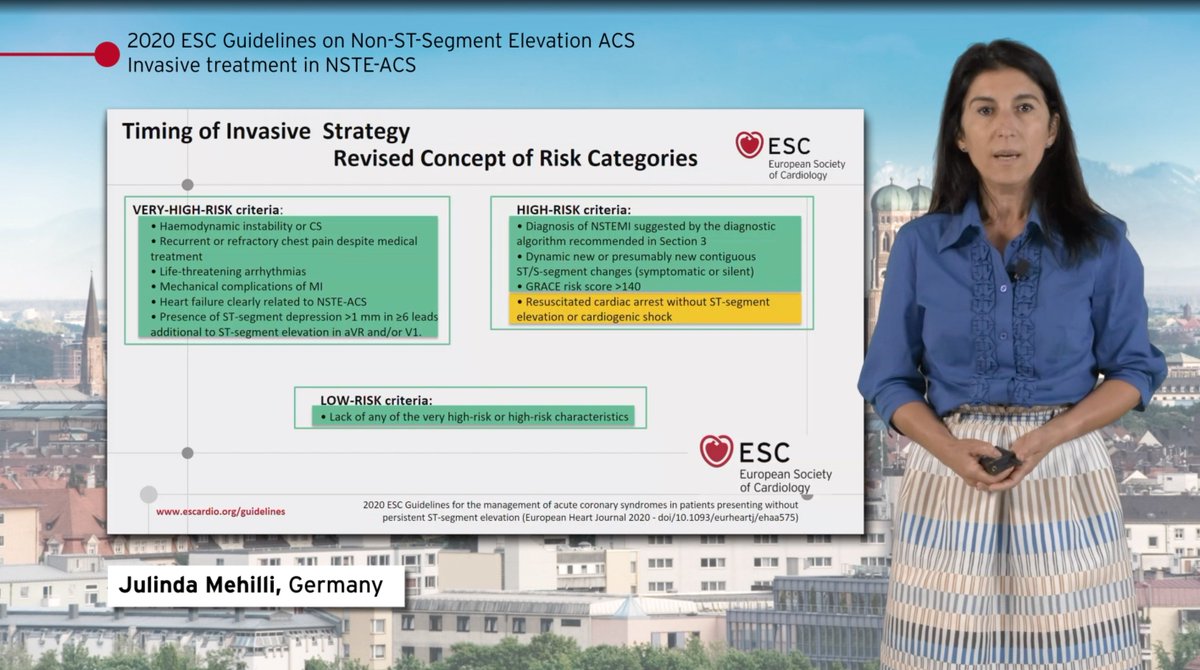
4/ Risk classifications
Very high risk: immediate PCI
High risk: <24h PCI
Low risk: non invasive stratification/transfer
Very high risk: immediate PCI
High risk: <24h PCI
Low risk: non invasive stratification/transfer

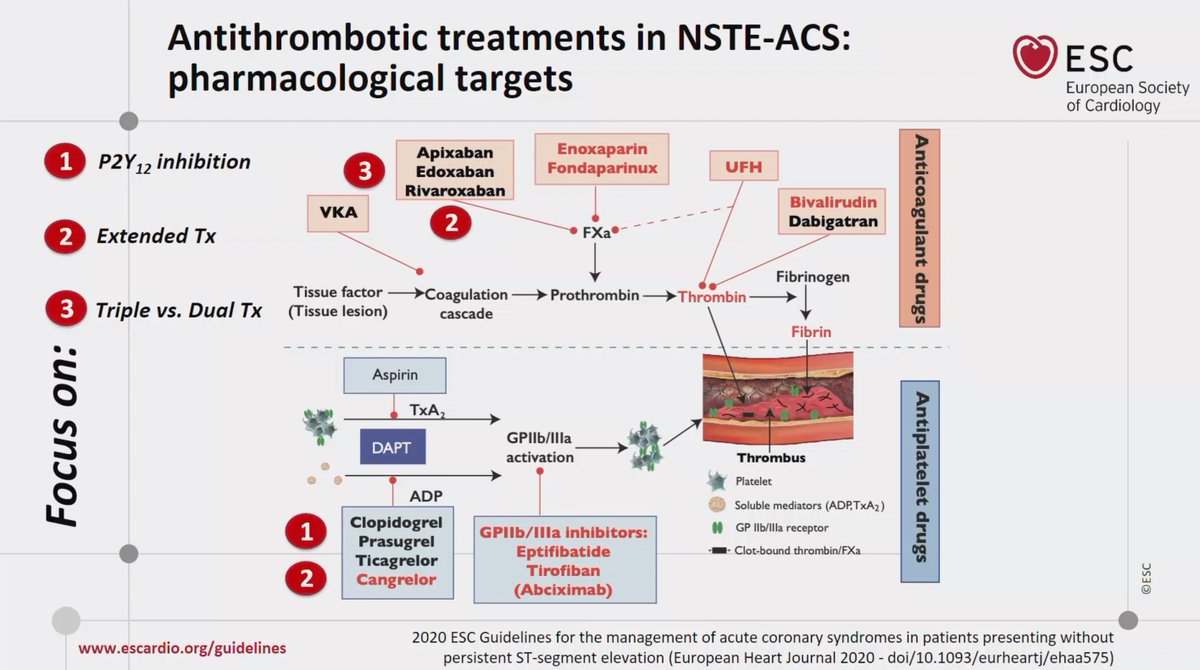
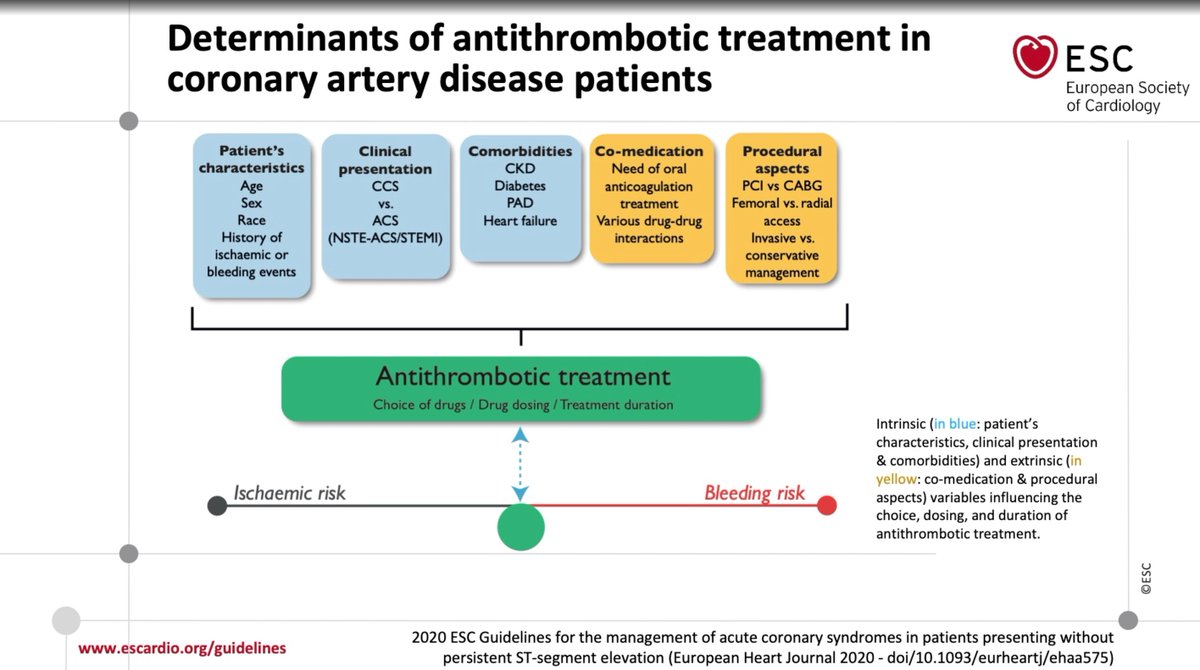
5/ Pharmacological treatment
Multiple therapeutic targets and combinations; individualization = key.
Patient characteristics, clinical presentation, comorbidities, co-medications and periprocedural aspects: determinants of treatment and rx duration.
Multiple therapeutic targets and combinations; individualization = key.
Patient characteristics, clinical presentation, comorbidities, co-medications and periprocedural aspects: determinants of treatment and rx duration.
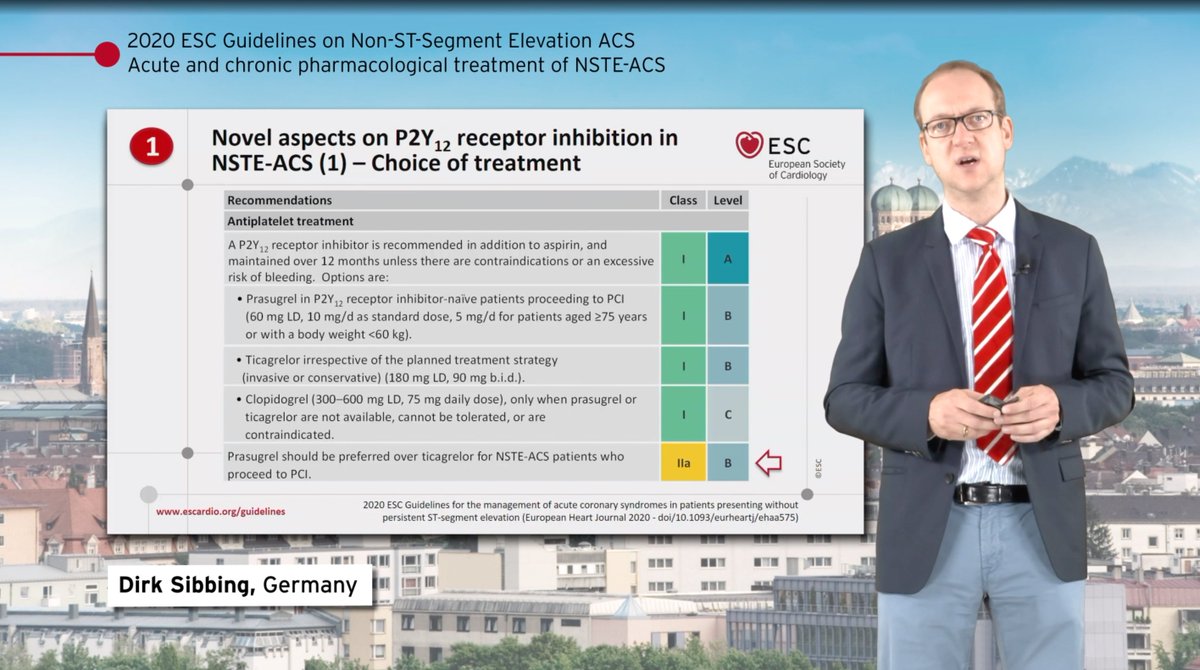
6/ Treatment recommendations
NOVEL: Prasugrel, first choice over Tica/Clopi (ISAR-REACT 5).. controversial!
NOVEL: not recommended to administer pre-treatment in patients planned to early invasive strategy (lack of evidence from ACCOAST, ISAR-REACT5)
NOVEL: Prasugrel, first choice over Tica/Clopi (ISAR-REACT 5).. controversial!
NOVEL: not recommended to administer pre-treatment in patients planned to early invasive strategy (lack of evidence from ACCOAST, ISAR-REACT5)


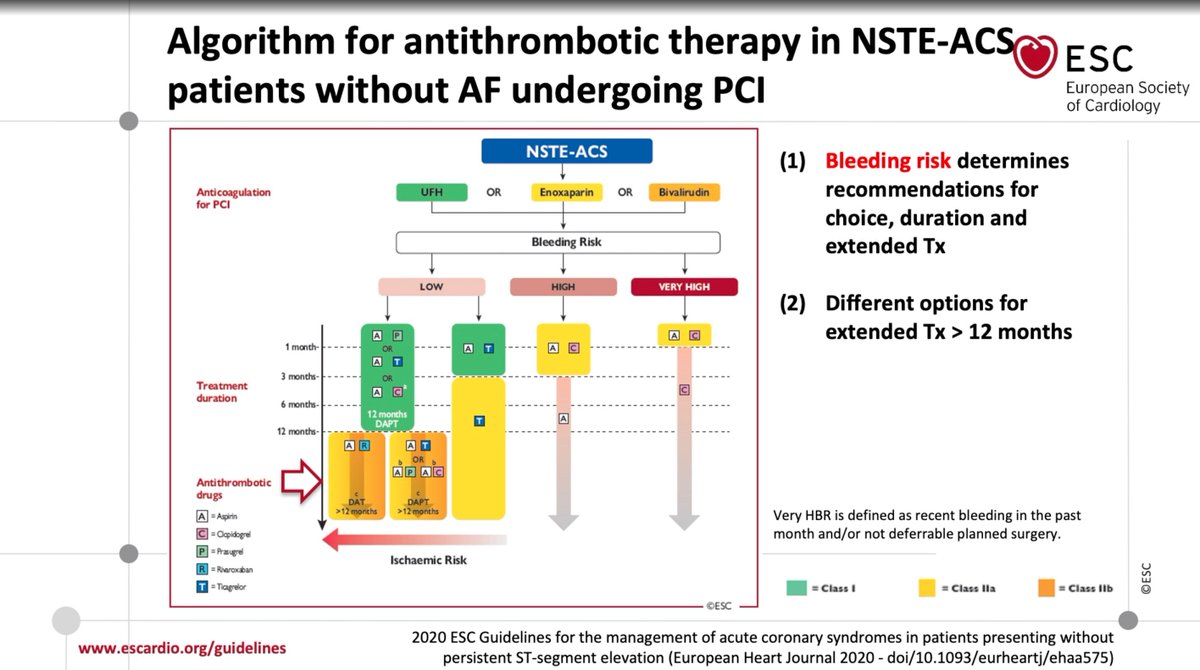
7/ Treatment combinations in patients with AF / duration of treatment:
- Bleeding risk determines, initially, the strategy.
- Ischemic risk may determine duration (particularly long term) of DAPT.
- DOAC+ p2Y12i combination of choice in AF
- Bleeding risk determines, initially, the strategy.
- Ischemic risk may determine duration (particularly long term) of DAPT.
- DOAC+ p2Y12i combination of choice in AF

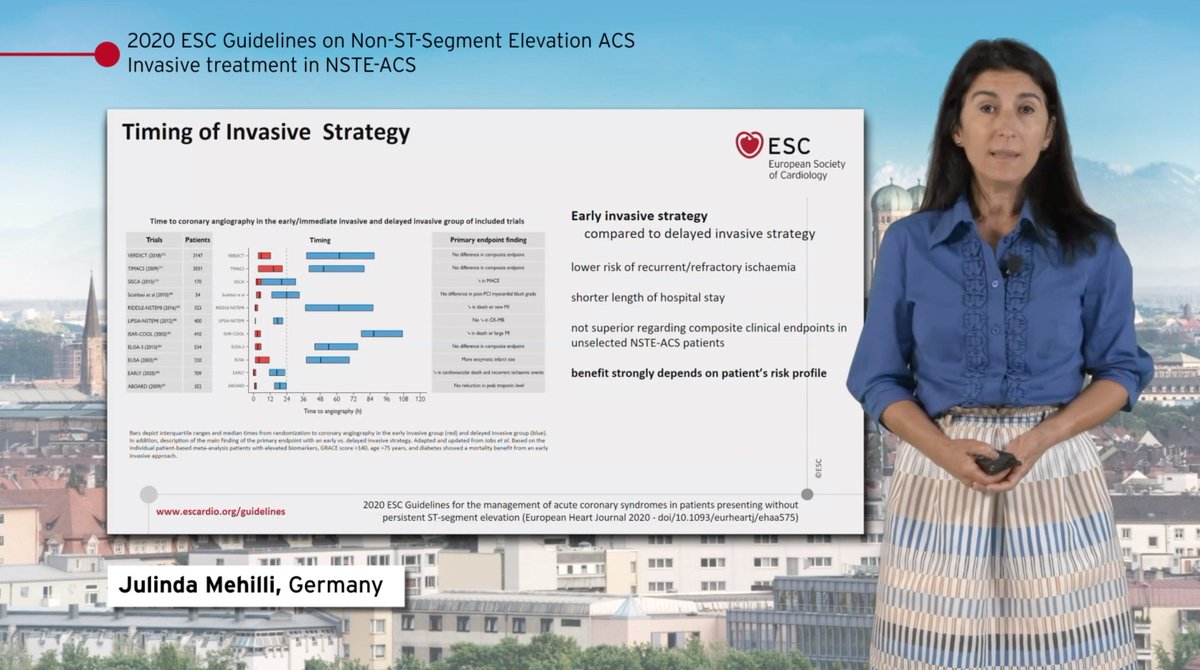
8/ Timing of invasive strategy
- Benefit of early invasive strategy correlates strongly with patient profile.
-- Very high risk: immediate PCI (<2h)
-- High risk: <24h
- Benefit of early invasive strategy correlates strongly with patient profile.
-- Very high risk: immediate PCI (<2h)
-- High risk: <24h

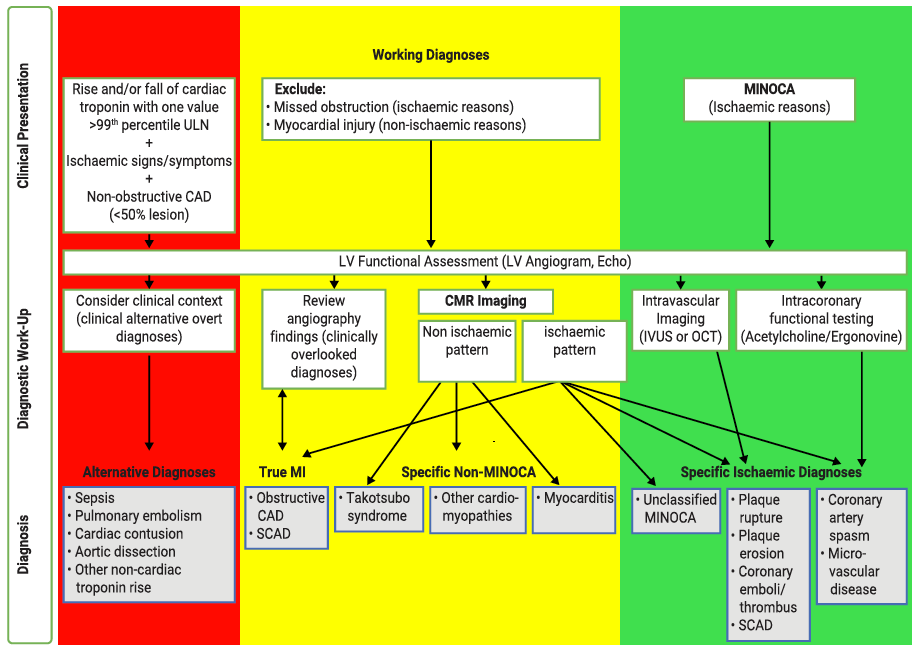
9/ New sections on SCAD related NSTEACS and MINOCA
- The importance of CMRi is highlighted in all patients with MINOCA
- Takotsubo is separated from MINOCA
- The importance of CMRi is highlighted in all patients with MINOCA
- Takotsubo is separated from MINOCA


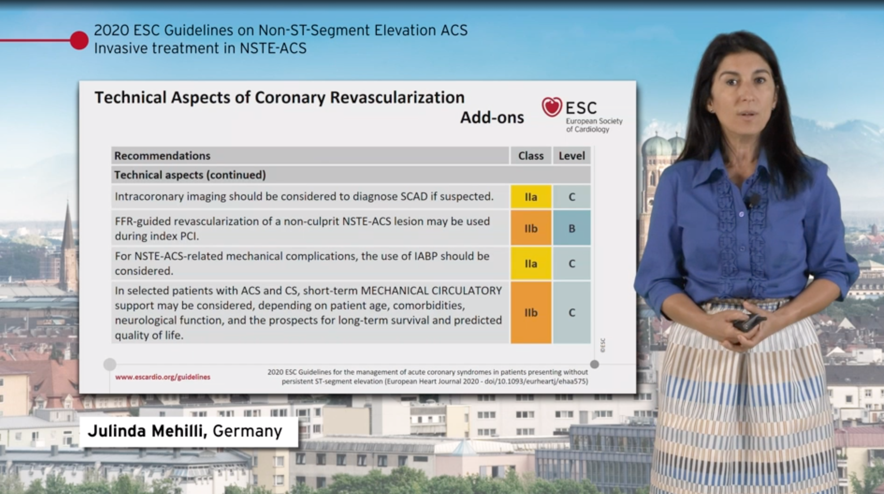
10/ Periprocedural aspects of PCI in NSTEMI
- FFR may be used to assess non culprit lesiones
- IABP IIaC, in mechanical complications
- MCS in ACS + CS: IIbC
- FFR may be used to assess non culprit lesiones
- IABP IIaC, in mechanical complications
- MCS in ACS + CS: IIbC
Thank you very much for reading! 👆🏼
@hvanspall @DrMarthaGulati @HanCardiomd @EkateriniL @AnastasiaSMihai @krychtiukmd @rafavidalperez @Hragy @thiele_holger @mmamas1973 @cpgale3 @cpcannon @clara_clarais @gonzaeperez @SIAC_cardio @smexcardiologia @berniann @AlcocerGamba
@hvanspall @DrMarthaGulati @HanCardiomd @EkateriniL @AnastasiaSMihai @krychtiukmd @rafavidalperez @Hragy @thiele_holger @mmamas1973 @cpgale3 @cpcannon @clara_clarais @gonzaeperez @SIAC_cardio @smexcardiologia @berniann @AlcocerGamba
• • •
Missing some Tweet in this thread? You can try to
force a refresh


