
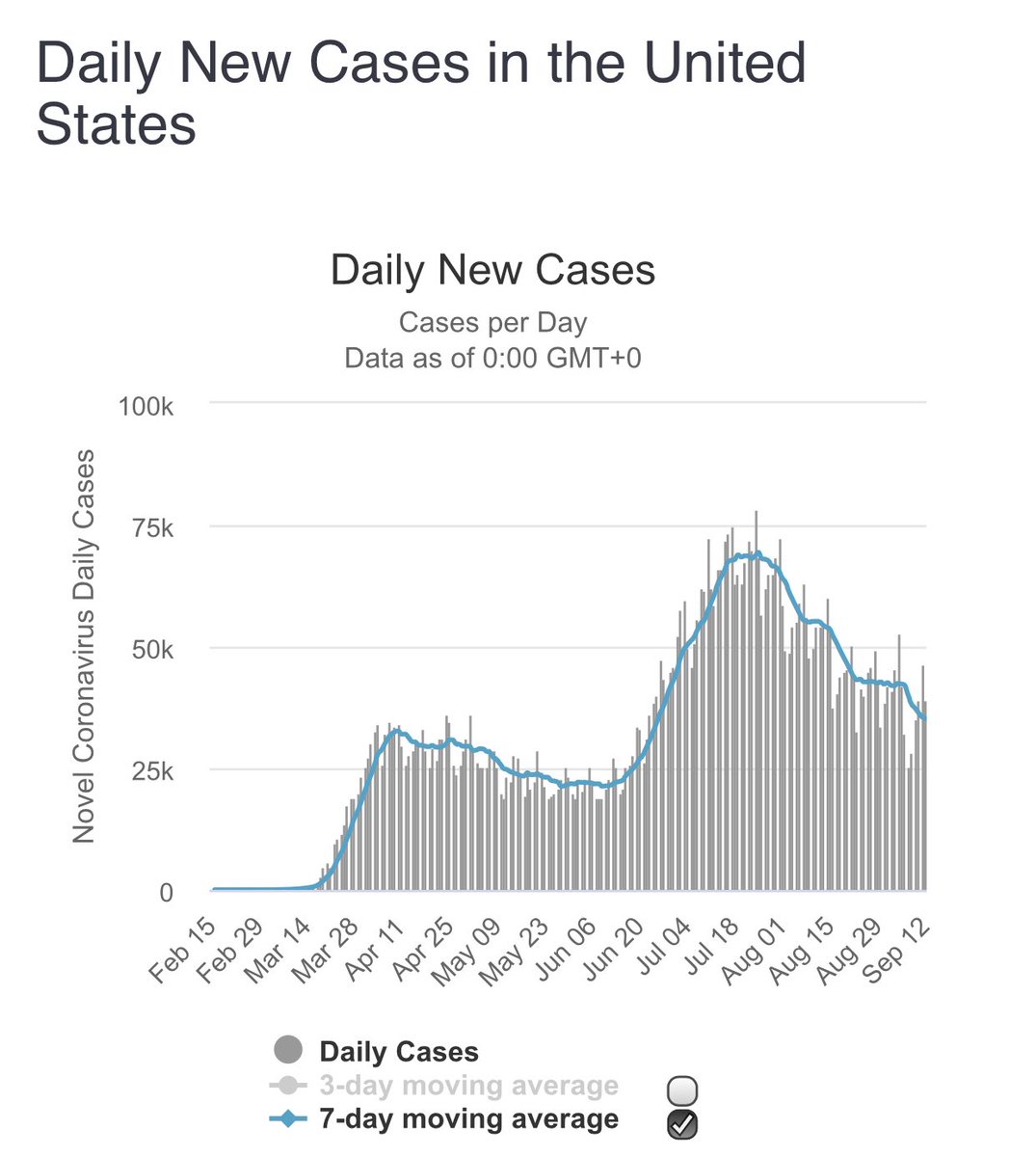
As I predicted a month ago the number of new COVID cases has decreased in the US. From a high of 70,000 per day to 35,000 per day now. It will likely continue to decrease for some more time.
This is due to many factors, but great national leadership is not one of them.
1/
This is due to many factors, but great national leadership is not one of them.
1/
Why are cases decreasing even though most of us are still susceptible?
2 reasons:
— Increasing proportion of persons at high risk of getting COVID (eg., jobs where u can’t social distance) have already had COVID
— Effect of masks & distancing
2/
2 reasons:
— Increasing proportion of persons at high risk of getting COVID (eg., jobs where u can’t social distance) have already had COVID
— Effect of masks & distancing
2/
But the proportion of people who have been exposed is very low even in hotspots. Less than 10%. Does this mean >90% of us are still susceptible? And if so, why are cases decreasing?
jamanetwork.com/journals/jamai…
3/
jamanetwork.com/journals/jamai…
3/

While we have to assume that we are all susceptible and continue to take preventive measures, seroprevalence studies likely underestimate the proportion of people who have been exposed to COVID. See article by @JoshuaPCohen1 @Forbes google.com/amp/s/www.forb…
4/
4/
But even if we do some rough math, and double the seroprevalence we will still have only estimated 10-15% of population as having been exposed to COVID, far lower than what is needed for true herd immunity, but yet cases are decreasing, even in many hot spots. Why?
5/
5/
Which brings us to the big question. Are we all equally susceptible to COVID? Or do some people have cross reactive immunity in which cases the disease is so mild that while you may get a PCR positive result, it doesn’t actually lead to symptoms or permanent seroconversion?
6/
6/
https://twitter.com/vincentrk/status/1278017849781563394
An important caveat:
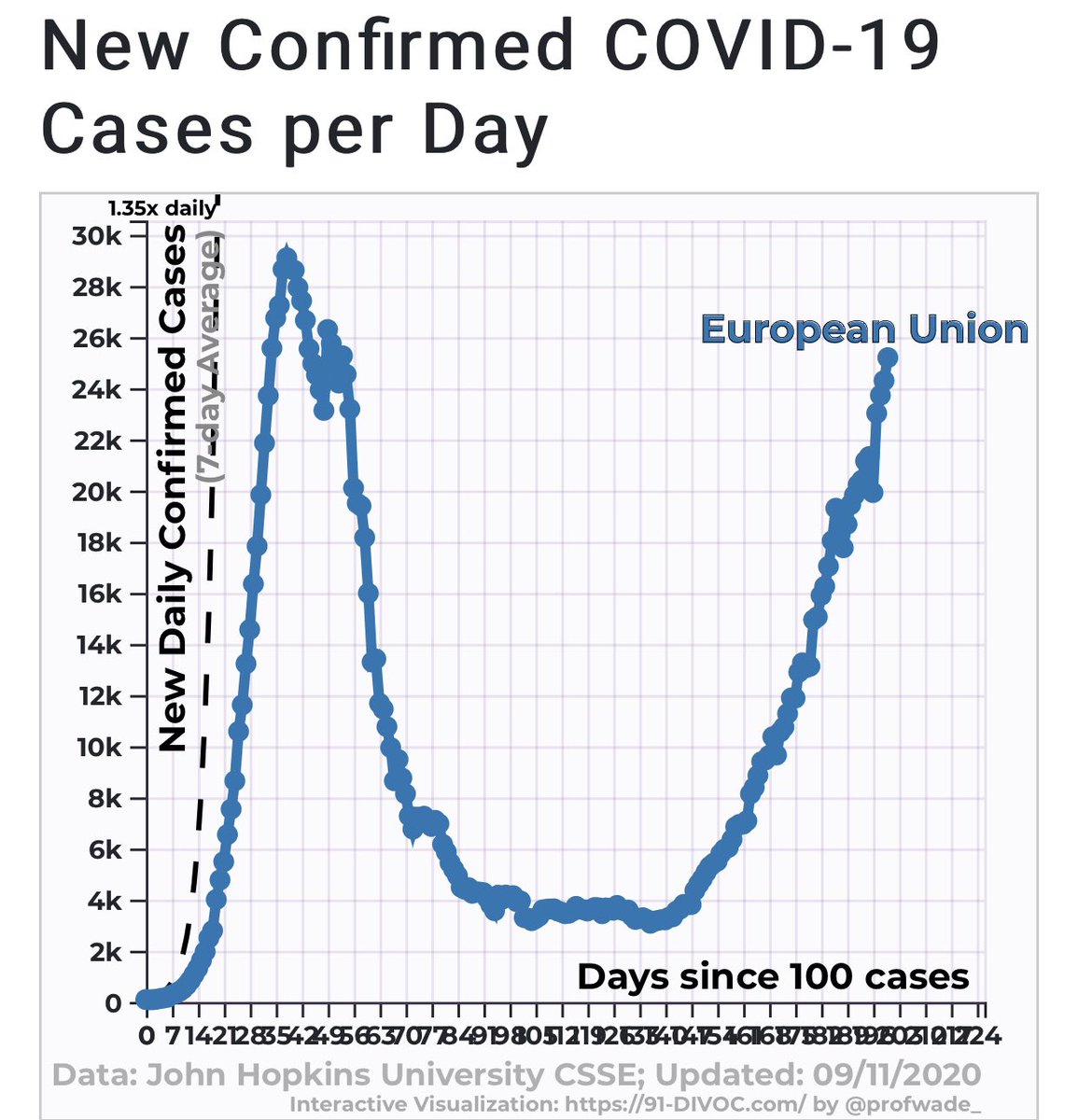
-What happens in Europe happens a month later in the US. In Europe there is a 2nd wave. Our cases can go up dramatically. We have to be careful & continue masks and social distancing because that may reduce viral dose and thereby the severity of COVID
7/
-What happens in Europe happens a month later in the US. In Europe there is a 2nd wave. Our cases can go up dramatically. We have to be careful & continue masks and social distancing because that may reduce viral dose and thereby the severity of COVID
7/
As cases come down leaders will naturally try to take credit. Or my worry is that they may tell people to relax. But to be clear the drop in cases is happening because of reduction in susceptible population and due to behavioral changes, specifically masks. @jeremyphoward
8/
8/
The number of daily cases now is higher than I thought it would have been at this point. But the trend is there.
https://twitter.com/vincentrk/status/1294968195829436416
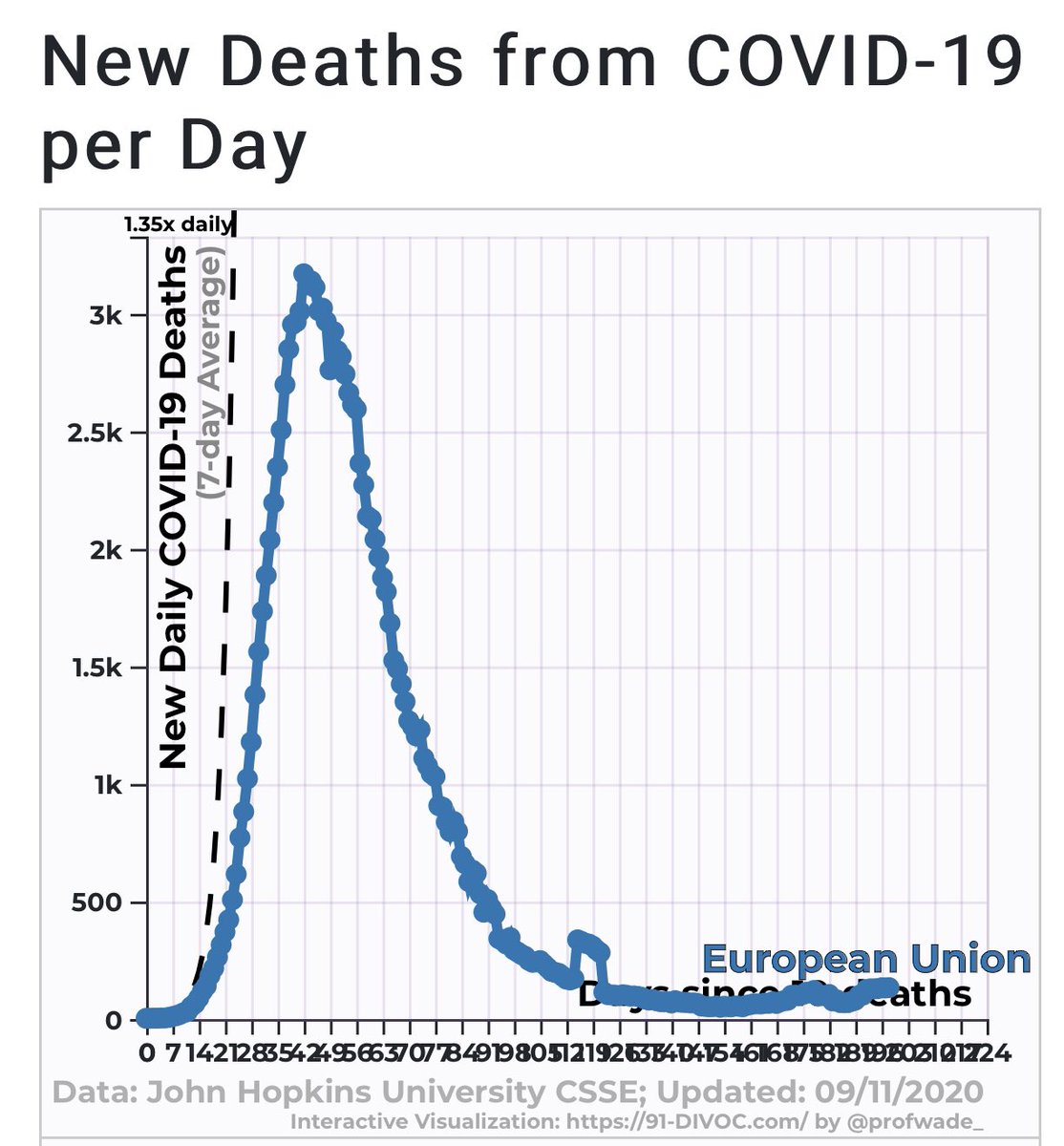
My feeling is that the drop in cases will be transient and we will have another peak in late fall. But my hope is that the drop in mortality is more enduring.
I also recognize that COVID has a lot of long term consequences. So it’s important we do everything to keep cases down
I also recognize that COVID has a lot of long term consequences. So it’s important we do everything to keep cases down
• • •
Missing some Tweet in this thread? You can try to
force a refresh


















