1/ Value-based care works. MSSP saved $2.6 billion dollars with $1.2 billion in net savings to Medicare, matching CBO’s savings expectations for 2019
Physician-led ACOs again out-performed hospital ACOs. What we need now is to help more practices participate in these models
Physician-led ACOs again out-performed hospital ACOs. What we need now is to help more practices participate in these models
https://twitter.com/Health_Affairs/status/1305570818949296128
2/ @AledadeACO is proud to be the largest, most successful nationwide enabler of physician-led ACOs, delivering better care at lower cost for >340,000 Medicare beneficiaries, saving Medicare and American taxpayers nearly $180 million in unnecessary health care spending last year!
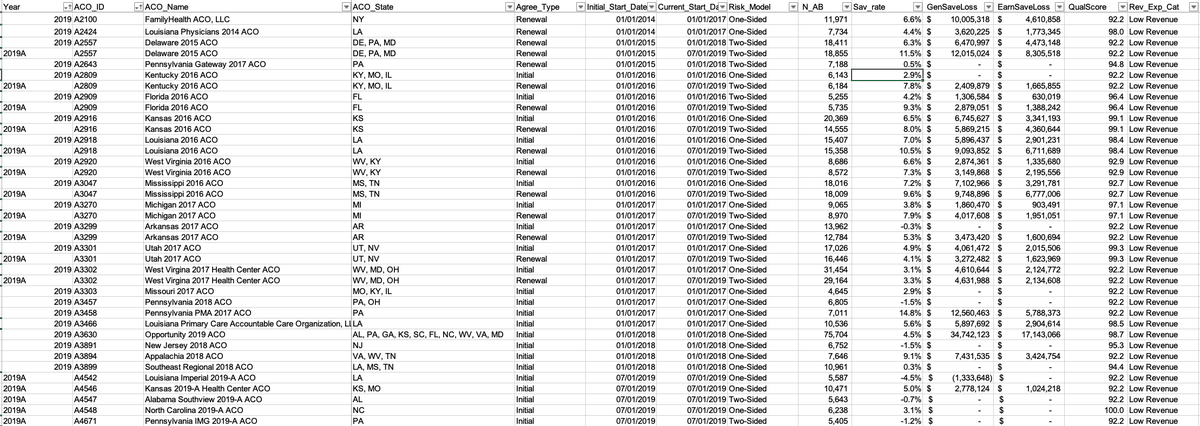
3/ Here's the list of the physician-led ACOs we are supporting, and our performance data.
* It doesn't matter if you're urban, rural, suburban, or in which state
* It gets better. The longer you work, the more the chances of success
* More risk = Higher rewards
* It doesn't matter if you're urban, rural, suburban, or in which state
* It gets better. The longer you work, the more the chances of success
* More risk = Higher rewards
4/ Last year was also the first year of the new Pathways to Success program. Every single one of Aledade’s MSSP ACOs who switched to Pathways to Success (higher risk/ higher reward) achieved savings. Every single one!
aledade.com/what-medicare-…
aledade.com/what-medicare-…
5/ Every Aledade ACO achieved an average quality score of 90% or higher for the year.
Our practices in MA earned ⭐️⭐️⭐️⭐️ in 2019, w many improving their rating by over a full ⭐️ since joining Aledade
As @SeemaCMS said- lower cost AND HIGHER QUALITY than Fee For Service
Our practices in MA earned ⭐️⭐️⭐️⭐️ in 2019, w many improving their rating by over a full ⭐️ since joining Aledade
As @SeemaCMS said- lower cost AND HIGHER QUALITY than Fee For Service

6/ Getting rid of hospital ACO squatters has not hurt the program savings, and has improved the numbers for the remaining "high revenue" ACOs.
But no matter where you look, legacy tracks or Pathways, one-sided, or two-sided, "low revenue" physician-led ACOs save TWICE as much
But no matter where you look, legacy tracks or Pathways, one-sided, or two-sided, "low revenue" physician-led ACOs save TWICE as much


7/ What's not great is that there are too few physician practices participating.
In California- land of capitation, >90% of small practices w fewer than 500 Medicare ACO lives, are not in an ACO model
We and @CMAdocs are working together to change that!
prnewswire.com/news-releases/…
In California- land of capitation, >90% of small practices w fewer than 500 Medicare ACO lives, are not in an ACO model
We and @CMAdocs are working together to change that!
prnewswire.com/news-releases/…
8/ "The trauma of the pandemic has underscored the need for a resilient health care system where reimbursement is not tied to volume of services provided, but rather to value-based incentives to keep patients healthy"
(We @AledadeACO are growing like crazy in the midst of COVID)
(We @AledadeACO are growing like crazy in the midst of COVID)
9/ We can least afford to lose practices in rural areas that are often the only source of primary care, and supporting them is a particular source of pride for us.
Giving advanced payments WORKED (AIM funding eval) innovation.cms.gov/data-and-repor…
CHART is putting more $ into them
Giving advanced payments WORKED (AIM funding eval) innovation.cms.gov/data-and-repor…
CHART is putting more $ into them

10/ But the best way to support rural physician-led ACOs is to be FAIR to them.
As it stands now, their lives are included in regional trends, which dilutes their true performance.
This "rural glitch" may account for virtually all of this discrepancy.
THIS HAS TO BE FIXED
As it stands now, their lives are included in regional trends, which dilutes their true performance.
This "rural glitch" may account for virtually all of this discrepancy.
THIS HAS TO BE FIXED

• • •
Missing some Tweet in this thread? You can try to
force a refresh