
#WorldSepsisDay
Time to move on from
"WHEN TO PRESCRIBE ANTIBIOTICS"
to
"WHEN TO RESIST THE TEMPTATION TO PRESCRIBE ANTIBIOTICS AND BE SAFE FOR THE PATIENT".
1/6
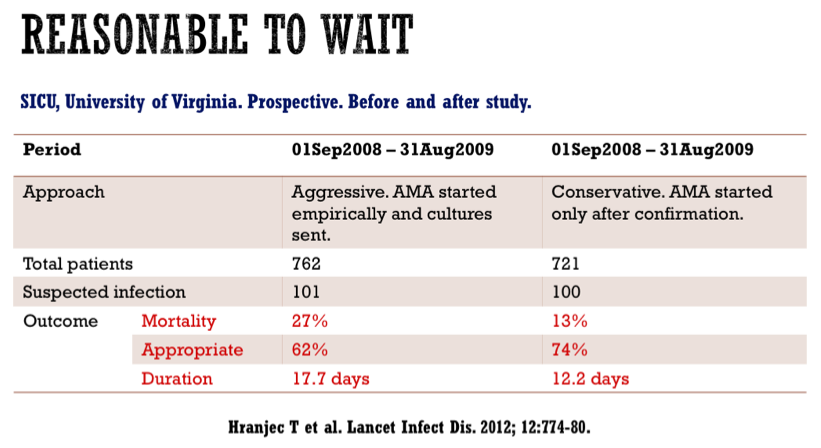
In most patients with exception of Septic Shock, we can wait for real evidence of infection and possible source.
Time to move on from
"WHEN TO PRESCRIBE ANTIBIOTICS"
to
"WHEN TO RESIST THE TEMPTATION TO PRESCRIBE ANTIBIOTICS AND BE SAFE FOR THE PATIENT".
1/6
In most patients with exception of Septic Shock, we can wait for real evidence of infection and possible source.
2/6
ED patients with LRTI and low suspicion of Bacterial Infection, it is reasonably safe to hold ABX if baseline PCT <0.25.
For additional safety, repeat PCT after 6-12 Hours for any rise.
In countries with high baseline antibiotic consumption, it can reduce ABX exposure.
ED patients with LRTI and low suspicion of Bacterial Infection, it is reasonably safe to hold ABX if baseline PCT <0.25.
For additional safety, repeat PCT after 6-12 Hours for any rise.
In countries with high baseline antibiotic consumption, it can reduce ABX exposure.


3/6
A low PCT value in appropriate clinical context is useful even in ICU patients to safely hold ABX.
Especially so in countries with high exposure to antibiotics.
PCT should not be used to escalate ABX [Jansen J U et al. Crit Care Med. 2011; 39:2048 –58].
A low PCT value in appropriate clinical context is useful even in ICU patients to safely hold ABX.
Especially so in countries with high exposure to antibiotics.
PCT should not be used to escalate ABX [Jansen J U et al. Crit Care Med. 2011; 39:2048 –58].

4/6
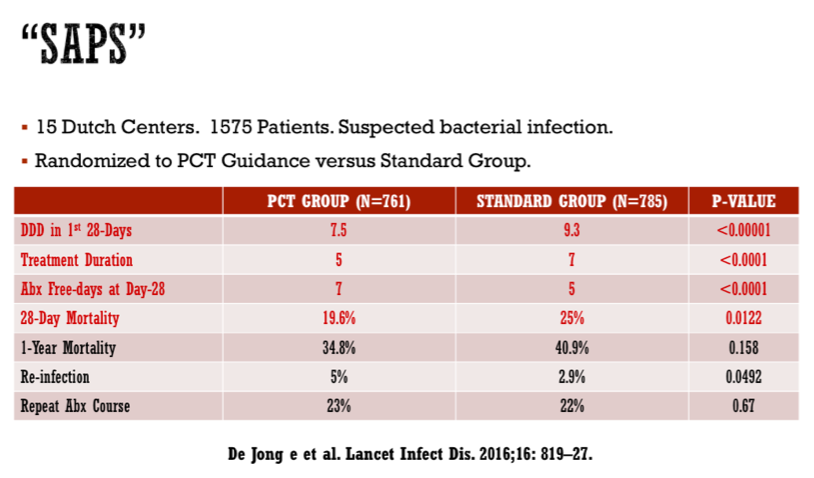
In most infections, short-course antibiotics is safe. But limited data available for all infections. Moreover, effect of antibiotics depends on host response. Needing a personalised antibiotic stopping rule.
PCT Algorithm is safe to discontinue ABX in a vast majority.
In most infections, short-course antibiotics is safe. But limited data available for all infections. Moreover, effect of antibiotics depends on host response. Needing a personalised antibiotic stopping rule.
PCT Algorithm is safe to discontinue ABX in a vast majority.

5/6
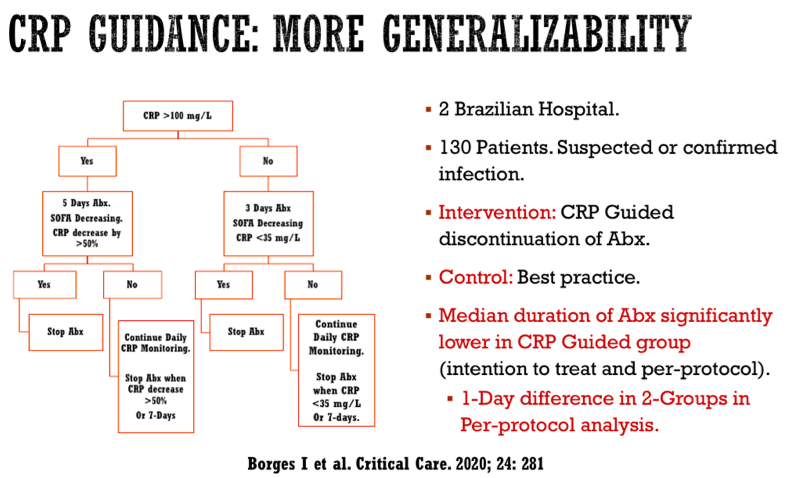
With high cost and sometimes non-availability of PCT, serial CRP can be used to stop ABX. Though the data is not as robust as PCT, relatively non-specific nature of CRP with slower dynamics.
With high cost and sometimes non-availability of PCT, serial CRP can be used to stop ABX. Though the data is not as robust as PCT, relatively non-specific nature of CRP with slower dynamics.

6/6
It is better to spend money on investigations and establish the diagnosis of bacterial infection. Then spend money on un-necessary antibiotics.
It is better to spend money on investigations and establish the diagnosis of bacterial infection. Then spend money on un-necessary antibiotics.

• • •
Missing some Tweet in this thread? You can try to
force a refresh


