Lots of discussion & opinions about human trials to test efficacy of vaccines. They provide key data to answer a Q that normal phase 3 trials can't:
Does the vaccine reduce infectiousness?
However, they have imp. limitations & carry risks.
Thread.
theguardian.com/world/2020/sep…
Does the vaccine reduce infectiousness?
However, they have imp. limitations & carry risks.
Thread.
theguardian.com/world/2020/sep…
Vaccines can reduce (mild or severe) disease (
who.int/blueprint/prio…
https://twitter.com/nataliexdean/status/1308474303810330625), reduce probability of infection, or reduce infectiousness/transmission. WHO criteria include all 3 of these as possible endpoints for vaccine efficacy.
who.int/blueprint/prio…
FDA criteria for efficacy include infection and disease (mild or severe), but nothing about infectiousness. This is problematic b/c we might think a vaccine is ineffective b/c it doesn't stop infection or reduce disease even if it reduces infectiousness enormously.
Many studies show no correlation b/w viral loads & disease severity, so this isn't an abstract possibility:
doi.org/10.1038/s41591…
doi.org/10.1038/s41591…
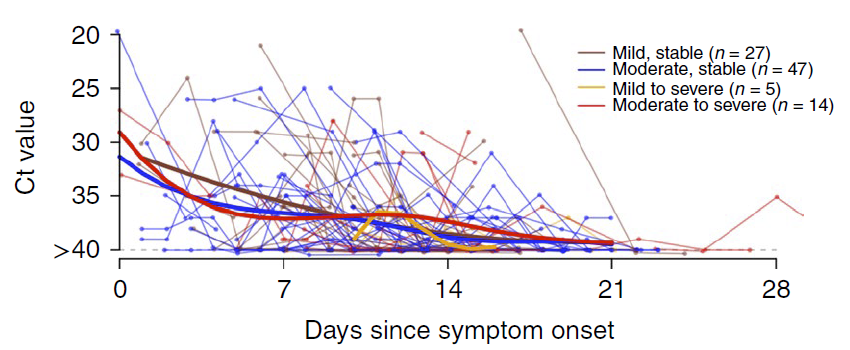
In a normal phase 3 trial with 30-60K people, one can't (easily) swab each person daily to get viral load data for the 150 infected people that constitute the endpoint. One could get daily viral load after symptom onset if participants seek testing at 1st symptom.
But, given importance of pre-symptomatic transmission (see our recent paper showing how it extends further into past if incubation period is longer:
https://twitter.com/LucaFerrettiEvo/status/1303302097455153153), we'd still miss this key part of transmission.

Challenge trials, with a small set of dozens of people, can easily measure viral loads on each day following infection, which is critical to determine if vaccination reduces infectiousness which could be completely missed by normal phase 3 trials.
Human challenge studies can also examine several factors phase 3 trials can't that are highly likely to be important: time of infection relative to vaccination, dose, etc. For dose effects see paper by
@ecoevo_kel
@mlipsitch
@mgmgomes1
nature.com/articles/s4159…
@ecoevo_kel
@mlipsitch
@mgmgomes1
nature.com/articles/s4159…
However, challenge trials aren't perfect: they are very limited in only including young healthy people, so they can't assess efficacy in older/sick people. They also certainly carry risks - COVID19 can (rarely) cause severe disease w/ lasting symptoms in young healthy people.
Many smart people are opposed to them for this reason
I acknowledge this risk, but believe it is outweighed by knowledge gained from trials.
https://twitter.com/florian_krammer/status/1309143153589579776
https://twitter.com/angie_rasmussen/status/1245804510028517377
I acknowledge this risk, but believe it is outweighed by knowledge gained from trials.
Some argue that normal phase 3 clinical trials provide the critical needed data on efficacy in older/sick people & simultaneously efficacy data in young people w/out ethical issue of deliberately infecting people.
But it's not clear to me that Phase 3 trials will provide this data; it's not clear the vaccine trial stopping criteria require a set of events in older people - do they @EricTopol @nataliexdean?). If not, they could stop w/out any info on efficacy in old/sick people.
So normal phase 3 trials and challenge trials might provide similar data. Why might we want to use both?
Phase 3 trials are difficult b/c you have to wait for enough people to accidentally get infected & get sick & come to doctor. To get efficacy they can take a long time, especially if transmission falls where you start a trial, as occurs very often.
Current trials focus on reducing mild illness which clearly isn't reason we urgently need vaccine for COVID. @EricTopol argues this is poor strategy b/c vaccine that prevents mild illness may have no effect on severe illness:
nytimes.com/2020/09/22/opi…
nytimes.com/2020/09/22/opi…
If we want phase 3 trial that assesses efficacy in preventing severe infections or specifically for old people, this will likely take many months.
In contrast, human trials can be completed in shorter time, once details of study are worked out (dose, timing relative to vaccination) & challenge virus is purified. Planned trials will take ~1 month to assess efficacy.
I believe human challenge trials are highly complementary to phase 3 trials and very valuable. They provide information on efficacy in reducing infectiousness that normal trials can't. They do carry risks. I support them.
Note: There are many many more vaccines in the pipeline (see article by @HelenBranswell), so just b/c some are in phase 3 now does not mean challenge trials won't be useful.
statnews.com/2020/09/24/her…
statnews.com/2020/09/24/her…
For very careful detailed discussion on pros/cons see paper from @mlipsitch from earlier this year:
https://twitter.com/mlipsitch/status/1245190118039867392
• • •
Missing some Tweet in this thread? You can try to
force a refresh