
School closures + bad science (THREAD)
Remember that 6 Apr Lancet C&AH systematic review on school closures--with that media-amplified "2-4%" statistic--by a UCL team led by RCPCH president + SAGE member Russell Viner?
It has some serious problems. 1/
thelancet.com/journals/lanch…
Remember that 6 Apr Lancet C&AH systematic review on school closures--with that media-amplified "2-4%" statistic--by a UCL team led by RCPCH president + SAGE member Russell Viner?
It has some serious problems. 1/
thelancet.com/journals/lanch…
Why does this still matter?
1. Viner's Review continues to be cited. A lot.
2. School closure was a first-aid response. Transitioning to long-term solutions calls for reexamining the science.
3. Serious enough cases of bad science raise concerns about the source. 2/
1. Viner's Review continues to be cited. A lot.
2. School closure was a first-aid response. Transitioning to long-term solutions calls for reexamining the science.
3. Serious enough cases of bad science raise concerns about the source. 2/
My first alarm bell?
The Review Summary's claim that "school closures alone would prevent only 2-4% of deaths" is a badly mis-contextualised statistic from
--wait for it--
the very Imperial College study [31] that prompted UK govt to close schools. 3/
imperial.ac.uk/media/imperial…
The Review Summary's claim that "school closures alone would prevent only 2-4% of deaths" is a badly mis-contextualised statistic from
--wait for it--
the very Imperial College study [31] that prompted UK govt to close schools. 3/
imperial.ac.uk/media/imperial…
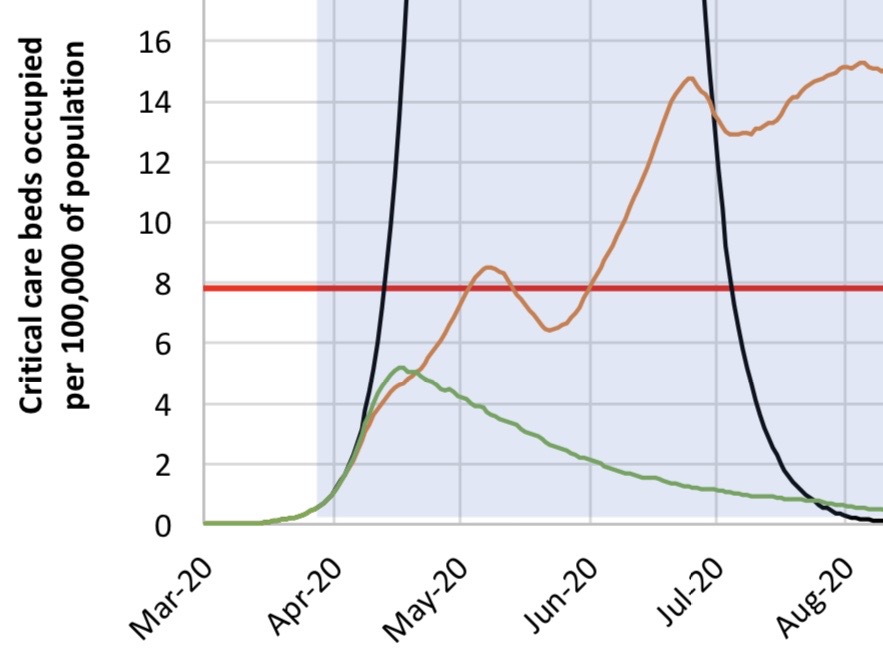
Viner's Review entirely omits the IC study's main predictions. Like that school closures would prevent 2-fold exceeding ICU bed capacity, with COVID only taking up a fraction of ICU beds.
Fig 3B (Red = ICU bed capacity, green vs brown = measures w/ vs w/o school closures.) 4/
Fig 3B (Red = ICU bed capacity, green vs brown = measures w/ vs w/o school closures.) 4/
Also omitted? The Summary never hints that all 5 of the Review's other included COVID-19 studies unanimously support school closures.
Still... most of the Review's included studies are used for their reference to the 2003 SARS epidemic.
That's where the real problems begin. 5/
Still... most of the Review's included studies are used for their reference to the 2003 SARS epidemic.
That's where the real problems begin. 5/
The Review's selection criteria insist on "quantitative studies" that "model or empirically evaluate" the impact of school-related measures on coronavirus spread.
But for 5 of their 9 included SARS studies, not a single datum they use has any bearing on the spread of SARS. 6/
But for 5 of their 9 included SARS studies, not a single datum they use has any bearing on the spread of SARS. 6/
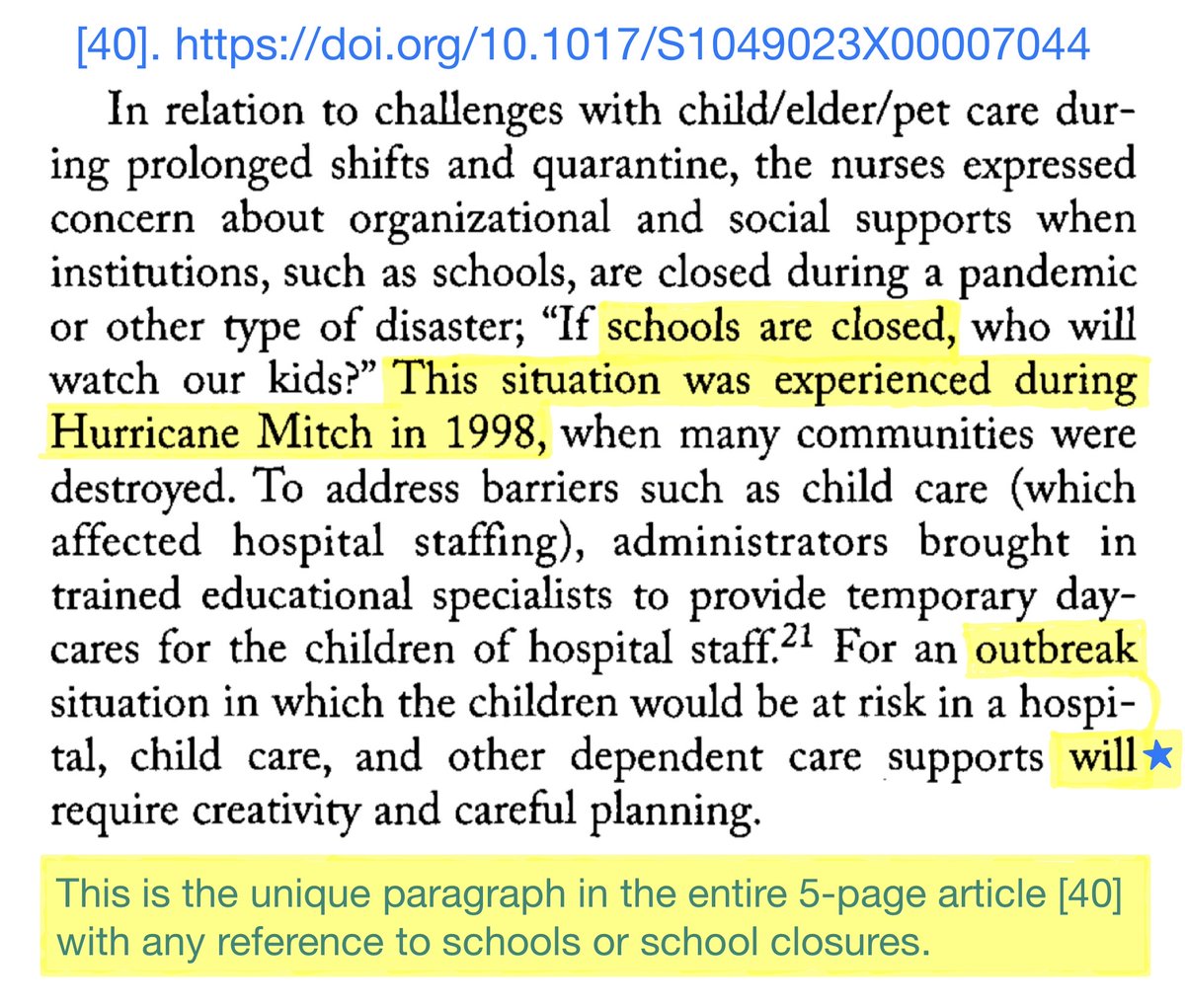
1 article is a 2008 qualitative survey of Canadian nurses on concerns about future epidemics.
Viner twice implies this article discussed nurse hardship caused by SARS 2003 school closures.
But that's false: with only 250 SARS cases, Canada didn't even *use* school closures. 7/
Viner twice implies this article discussed nurse hardship caused by SARS 2003 school closures.
But that's false: with only 250 SARS cases, Canada didn't even *use* school closures. 7/
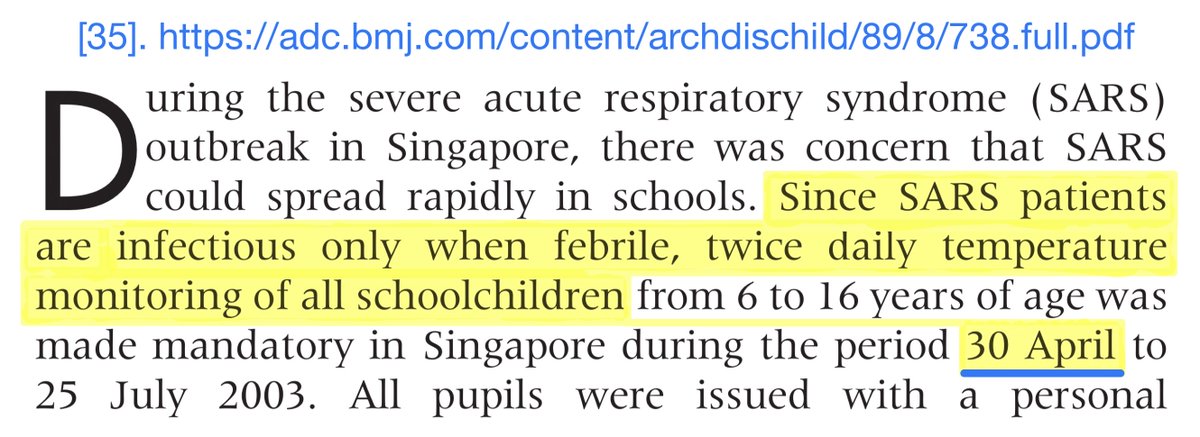
For 2+3 [34,35], Viner *solely* uses remarks about a Singapore school temperature-screening programme not finding any SARS.
Except: the epidemic was already over by then!
School temp screening started 30 Apr. Last 3 cases ever of that Singapore epi were 25&27 Apr + 5 May. 8/
Except: the epidemic was already over by then!
School temp screening started 30 Apr. Last 3 cases ever of that Singapore epi were 25&27 Apr + 5 May. 8/
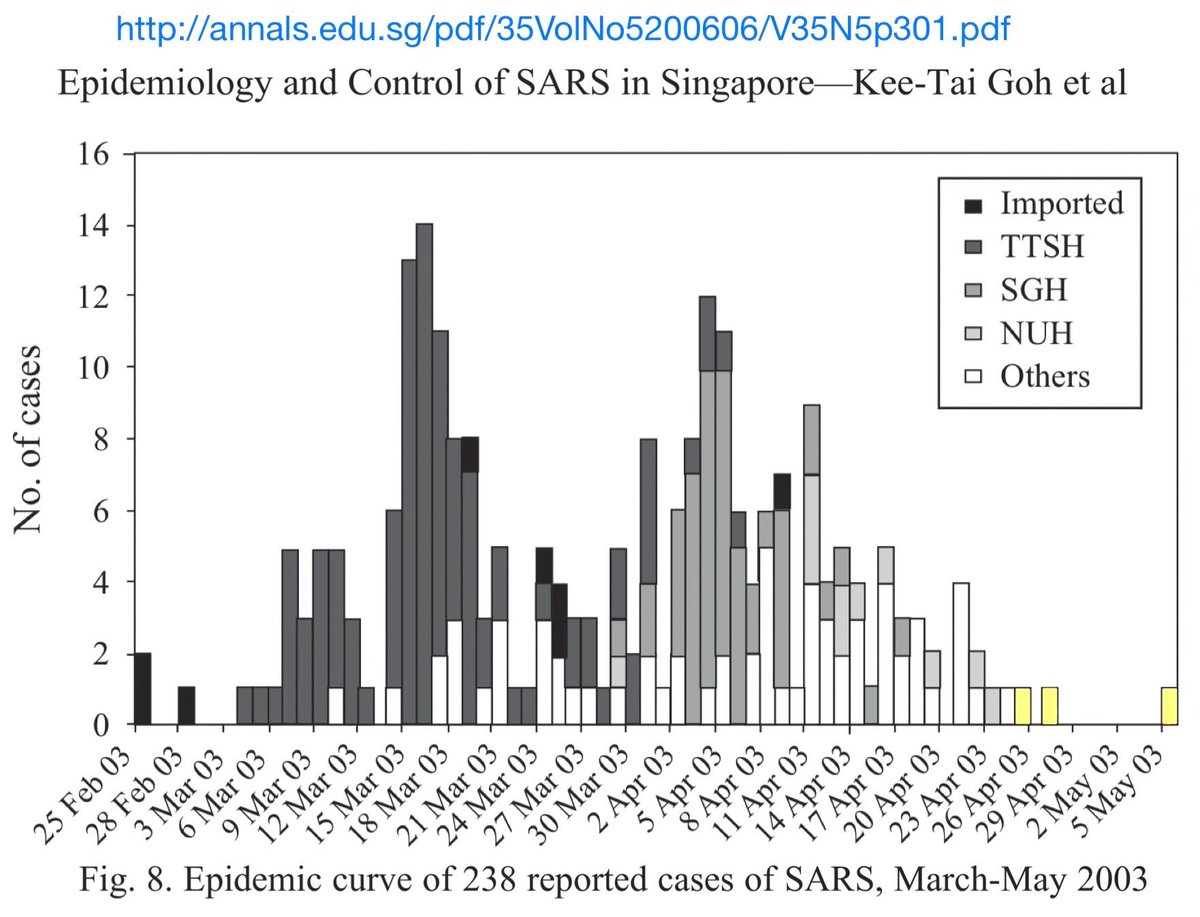
The above-right chart isn't cited in the Review. In fact, no articles that provide or analyse SARS case-count timelines for Toronto/Canada, Singapore, Taiwan, or Hong Kong are cited in Viner's Review, even for reference.
Easy to find, tho. Like this: 9/
ncbi.nlm.nih.gov/books/NBK92467/
Easy to find, tho. Like this: 9/
ncbi.nlm.nih.gov/books/NBK92467/
For 4th article, Viner only reports that schools and activities closed in Singapore “for 3 weeks from Mar 27" for an outbreak "from late Feb to May 2003.”
Except: Feb+May had only 4 cases total. Closures started at height of the epi, +ended with avg daily case counts at 2-3. 10/
Except: Feb+May had only 4 cases total. Closures started at height of the epi, +ended with avg daily case counts at 2-3. 10/
5th [24] is a 2014 Taiwanese systematic review on planning for future epidemics.
Every single SARS-related statement Viner's Review makes about this article is false.
In fact, this article never spoke of *anything* related to schools from *during* the 2003 SARS epidemic. 11/
Every single SARS-related statement Viner's Review makes about this article is false.
In fact, this article never spoke of *anything* related to schools from *during* the 2003 SARS epidemic. 11/
All 5 of these articles meet multiple exclusion criteria, often even for genre. For instance [34]+[24] are (allegedly-excluded) systematic reviews. And the Review's only use of [34] is duplicated by [35], which was cited by [34].
Even so... the problems have only begun. 12/
Even so... the problems have only begun. 12/
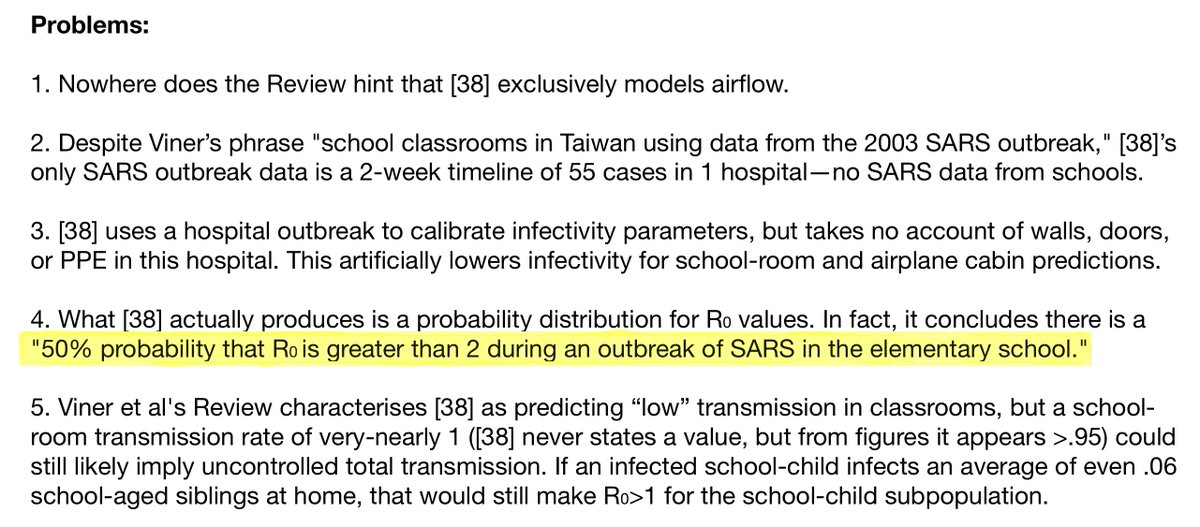
6th [38] is an airflow-modelling study predicting infection rate by droplets from 1 SARS-contagious person in a hospital, school room, or airplane, distinguished only by ventilation +occupancy rates.
More relevant than prior SARS studies, but still has problems (see inset). 13/
More relevant than prior SARS studies, but still has problems (see inset). 13/
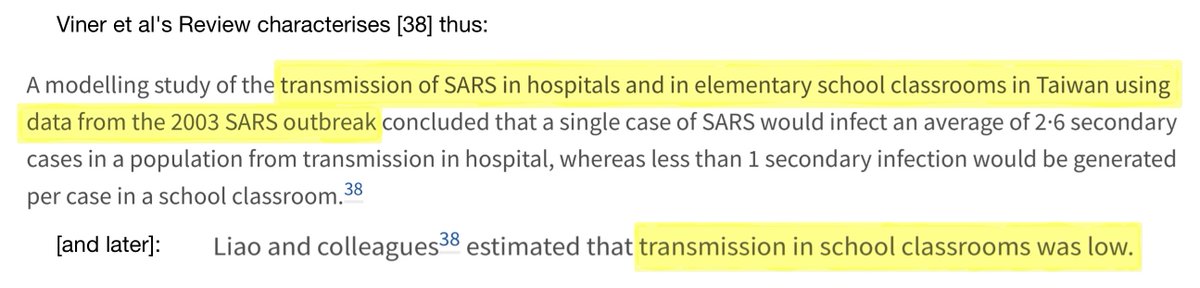
7+8 [36,37], on Beijing, finally use SARS outbreak data!
The Review correctly reports these studies' scepticism on the utility of school closure,
but fails to mention their scepticism on:
closure of public places, travel checkpoint screening, +quarantine of low-risk cases. 14/
The Review correctly reports these studies' scepticism on the utility of school closure,
but fails to mention their scepticism on:
closure of public places, travel checkpoint screening, +quarantine of low-risk cases. 14/
In fact, they predicted healthcare facility improvements + high-risk contact tracing alone were sufficient to stop SARS.
How could this be?
Because SARS DIDN'T HAVE A/PRE-SYMPTOMATIC TRANSMISSION.
SARS was completely eradicated before exceeding 8500 cases ever, worldwide. 15/
How could this be?
Because SARS DIDN'T HAVE A/PRE-SYMPTOMATIC TRANSMISSION.
SARS was completely eradicated before exceeding 8500 cases ever, worldwide. 15/
Consider: Beijing hosted 30% of the world’s SARS cases, with 90% concentrated in one month.
The avg of the 7 *highest* SARS daily case counts for Beijing was still *lower* per population than the UK's LOWEST EVER 7-day-moving-avg COVID-19 daily case count since late March. 16/
The avg of the 7 *highest* SARS daily case counts for Beijing was still *lower* per population than the UK's LOWEST EVER 7-day-moving-avg COVID-19 daily case count since late March. 16/
This transmission distinction for SARS v COVID was raised in a UK SAGE document in January and confirmed in multiple high-impact peer-reviewed studies in February.
The Review somehow skips over its cited articles' frequent allusions to this aspect of SARS.
But I digress. 17/
The Review somehow skips over its cited articles' frequent allusions to this aspect of SARS.
But I digress. 17/
9th [39] is an Australian modelling study supporting school closures, which the Review does its best to de-emphasise.
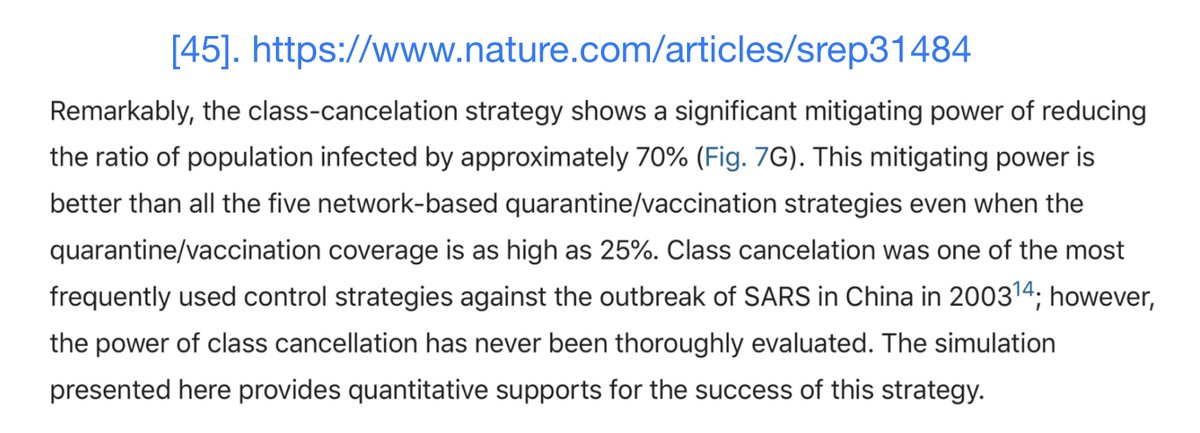
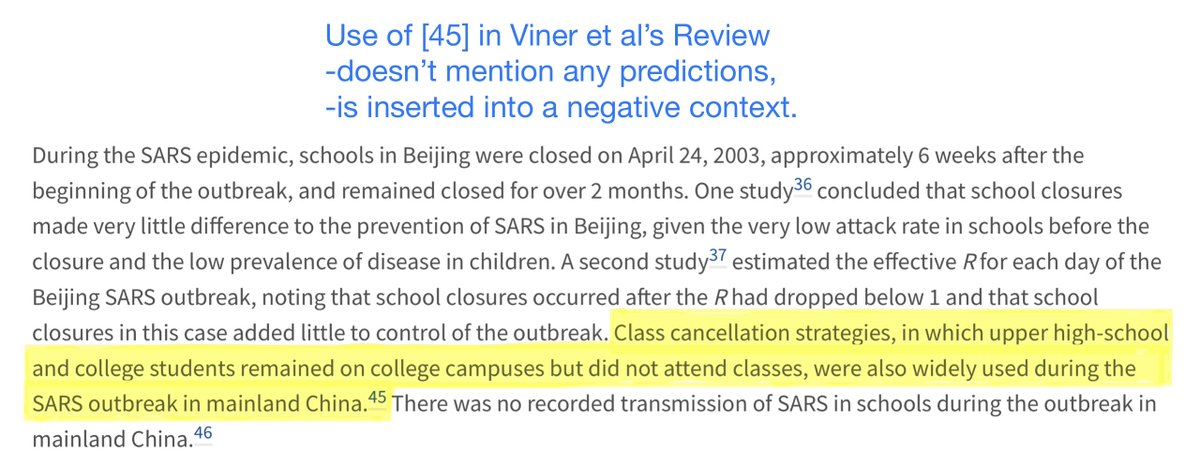
OTOH, the Review entirely omits the main prediction--a 70% reduction in infections--from a conveniently-excluded, but cited, class cancellation study [45]. 18/
OTOH, the Review entirely omits the main prediction--a 70% reduction in infections--from a conveniently-excluded, but cited, class cancellation study [45]. 18/
It also omits 2 pro-school-closures COVID-19 studies from February that contrast control measures with vs without school closures,
despite implying no such studies exist, and despite these studies fitting selection criteria. 19/
doi.org/10.1101/2020.0…
doi.org/10.1101/2020.0…
despite implying no such studies exist, and despite these studies fitting selection criteria. 19/
doi.org/10.1101/2020.0…
doi.org/10.1101/2020.0…
It also inserts a defacto 2nd systematic review on influenza into the Discussion section, but without stating selection criteria, and without providing crucial context, without which statistics are destined to be misinterpreted in a way that biases against school closures. 20/
It also alters data from a Hong Kong study [27], changing the stated primary source of pediatric SARS infection
from hospital spread plus an infected aerosol from leaky plumbing at the Amoy Gardens apartment complex
to spread "almost entirely through family settings." 21/
from hospital spread plus an infected aerosol from leaky plumbing at the Amoy Gardens apartment complex
to spread "almost entirely through family settings." 21/
Meanwhile, Viner, still on SAGE, is fighting against masks in schools 22/
https://twitter.com/BBCNewsnight/status/1298021228146495492?s=20
Science this problematic requires action.
/ENDS
/ENDS
• • •
Missing some Tweet in this thread? You can try to
force a refresh









