
Depletion of surfactant from the lungs of rats followed by mechanical ventilation is sufficient to cause infiltration by neutrophils, tissue damage, and pneumocyte apoptosis.
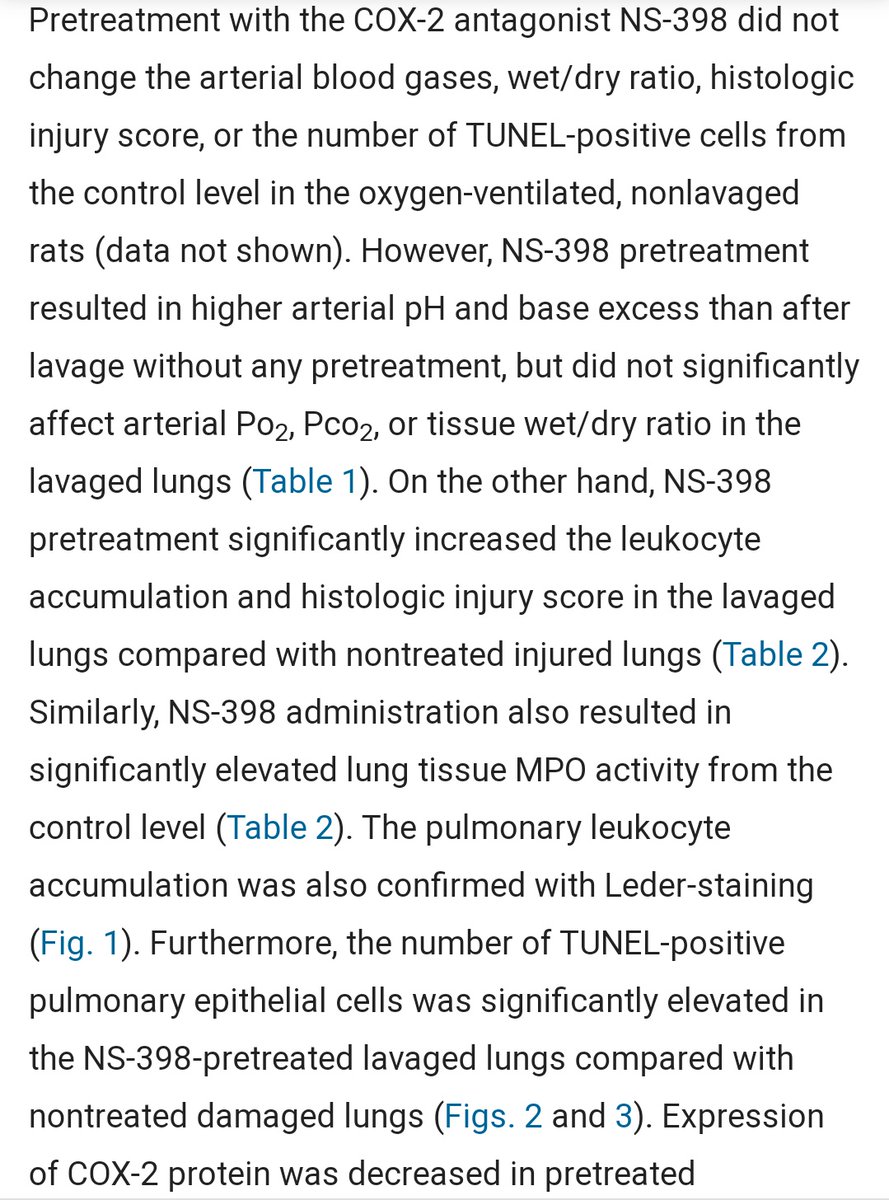
COX-2 expression was reduced, and treatment with COX-2 inhibitors further worsened the resulting damage.
COX-2 expression was reduced, and treatment with COX-2 inhibitors further worsened the resulting damage.
https://twitter.com/mozfart/status/1309830532931428355


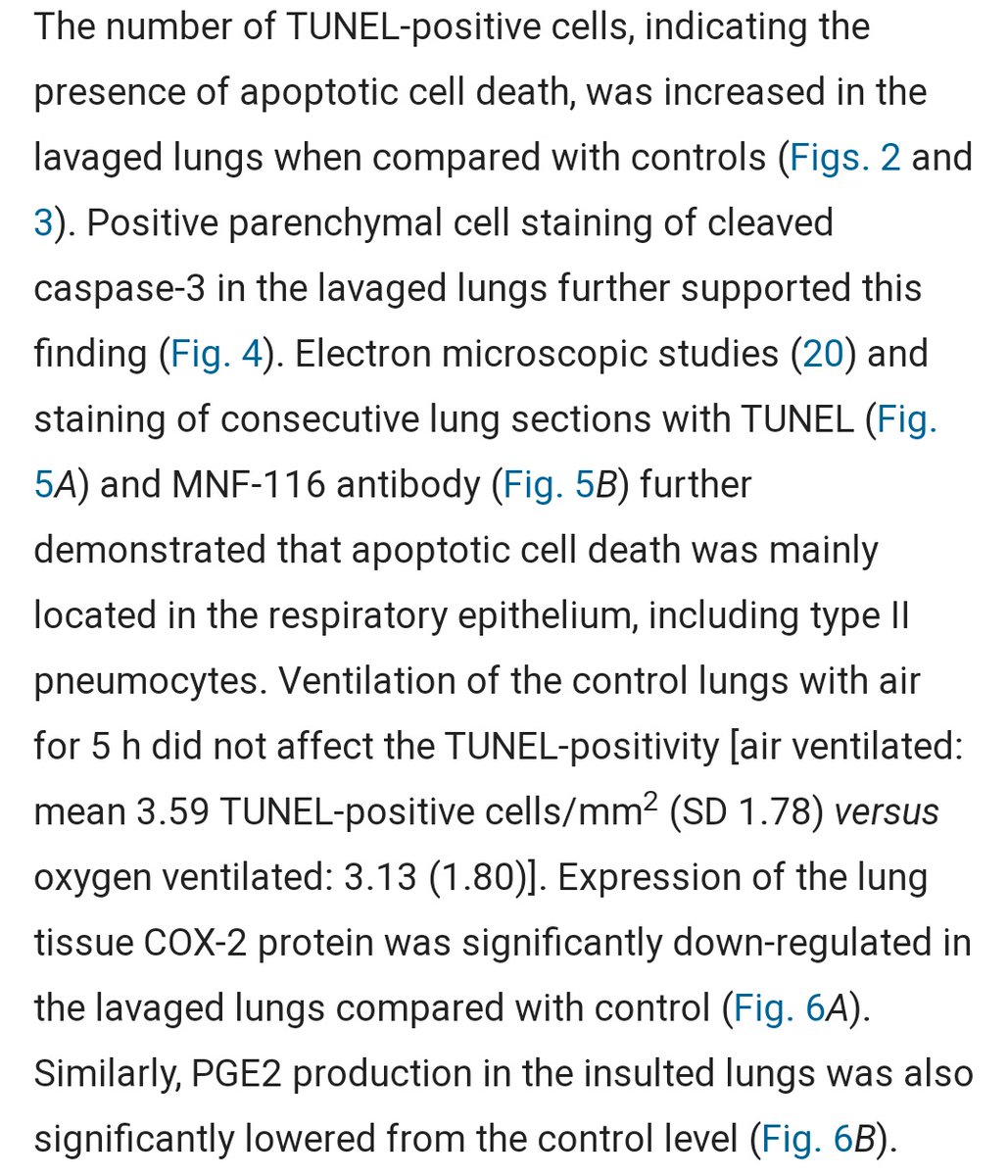
Histological samples resemble autopsies from fatal COVID-19, with extensive alveolar exudates, epithelial cell apoptosis, and neutrophil infiltration.
SARS-CoV-2 destroys secretory cells, reducing surfactant production and thereby promoting the above. Replace the surfactant.
SARS-CoV-2 destroys secretory cells, reducing surfactant production and thereby promoting the above. Replace the surfactant.
COX-2 inhibitors further increased the damage. Most aren't used often anymore, as they were infamously associated with cardiovascular disease.
The reason is likely their mitochondrial toxicity, especially harmful under conditions of intense stress.
sciencedirect.com/science/articl…
The reason is likely their mitochondrial toxicity, especially harmful under conditions of intense stress.
sciencedirect.com/science/articl…


This seems to raise questions about e.g. indomethacin in moderate to severe cases, but it is difficult to know without trial data.
pubmed.ncbi.nlm.nih.gov/12123755/
The issue appears less likely to be relevant in milder cases, if it is indeed a potential concern. Opinions welcome.
pubmed.ncbi.nlm.nih.gov/12123755/
The issue appears less likely to be relevant in milder cases, if it is indeed a potential concern. Opinions welcome.
@SWICU_Rays I thought of your recent experiments when I saw this. Another nice model for extracting a single facet of the COVID-19 disease process-- in this case, surfactant removal. Note the extensive alveolar damage and neutrophils.
@farid__jalali @pathdoc3 resembles earlier discussions on inadequate surfactant in hyaline membrane disease, another model converging on the same conclusion apart from the known case of infant respiratory distress syndrome
• • •
Missing some Tweet in this thread? You can try to
force a refresh
















