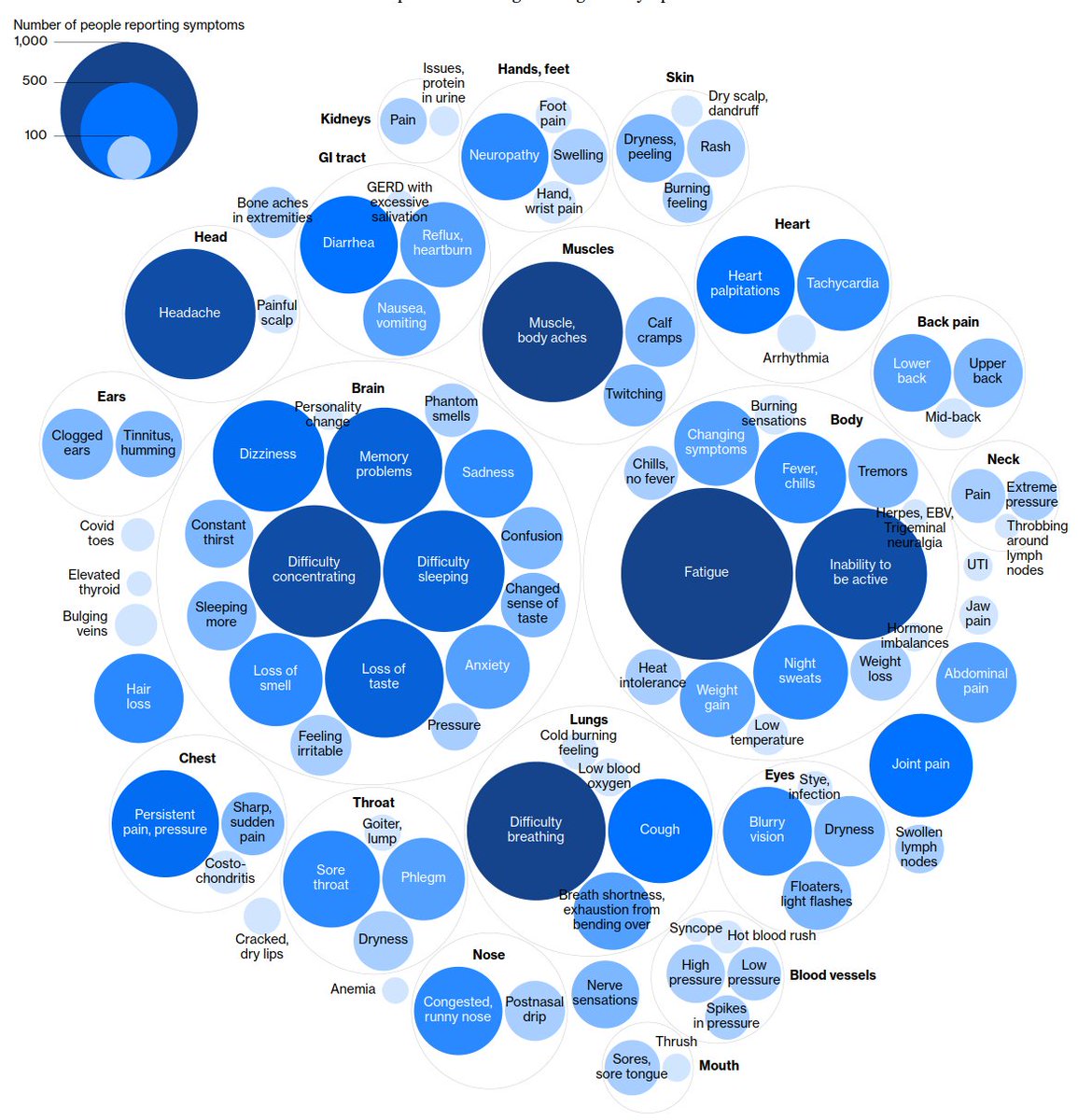
The attention-grabbing data shown in this Bloomberg article is data described as being collected from "1500 patients".
bloomberg.com/graphics/2020-…
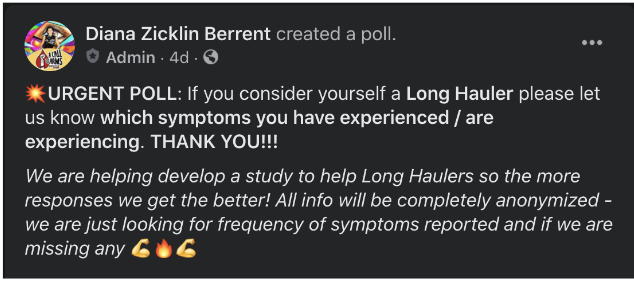
In fact, recruitment to this study was done via the social media post shown below.
The long-term burden of COVID infections is... 1/4
bloomberg.com/graphics/2020-…
In fact, recruitment to this study was done via the social media post shown below.
The long-term burden of COVID infections is... 1/4
an important scientific question.
We are not making progress on this question by overemphasizing the role of anecdotes
There is no technical reason why this cannot be answered using a scientific approach. A random sample of past COVID+ patients should be surveyed... 2/4
We are not making progress on this question by overemphasizing the role of anecdotes
There is no technical reason why this cannot be answered using a scientific approach. A random sample of past COVID+ patients should be surveyed... 2/4
and examined at 3 months, 6 months, etc, and proper comparisons should be made (e.g., to other respiratory infections).
We are 9 months into the pandemic.
The importance we place on this problem should be reflected in the seriousness with which we approach it. 3/4
We are 9 months into the pandemic.
The importance we place on this problem should be reflected in the seriousness with which we approach it. 3/4
Inaccurate information in itself incurs health costs.
Before amplifying anecdotes, I would ask scientists to imagine an experiment in which we randomize people receiving COVID test results to read "long COVID" stories.
Would we expect no negative effects on health and QOL? 4/4
Before amplifying anecdotes, I would ask scientists to imagine an experiment in which we randomize people receiving COVID test results to read "long COVID" stories.
Would we expect no negative effects on health and QOL? 4/4
• • •
Missing some Tweet in this thread? You can try to
force a refresh