
More data on schools in GA. I am trying to do comparisons that are reasonably near each other geographically, and have a difference in virtual vs in-person school. First up, Gwinnett (Aug start school) vs Dekalb Co. (virtual) 1/ 


Second up, our coastal region. Chatham Co is virtual, while Effingham,Bryan,Liberty,Mcintosh,Glynn have some in person options with varied Aug start dates. Will try to add more to this today. 2/


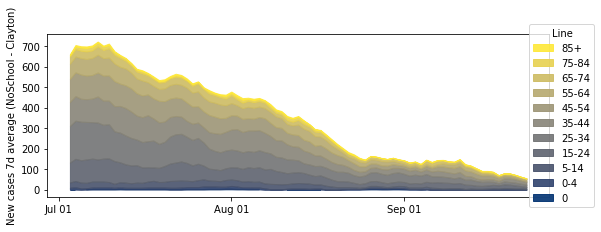
Clayton County, no school. Fayette County with a Aug 17 start. (note: population of Clayton is larger).

Cobb County (still virtual) vs Forsyth+Cherokee counties (in person Aug 1 in Cherokee and Aug 17 in Forstyth). Most in person also have virtual option.


Add up all the counties in this thread, with some effort to pair them geographically and by population. I get school in session with Rt of 0.83 and school virtual with Rt of 0.85. Calculations from mid-Aug to mid-Sept using 6.5 day cycle.


Conclusions: the introduction of managed in-person school with restrictions in Georgia has not resulted in obvious measurable spread. School systems that are virtual should migrate to careful, managed, in person options asap. Masks, and outdoor options, especially!
@threadreaderapp unroll, please
• • •
Missing some Tweet in this thread? You can try to
force a refresh










