Now that folks have had a chance to digest the two reports on in-hospital cardiac arrest in COVID patients, let’s break them down.
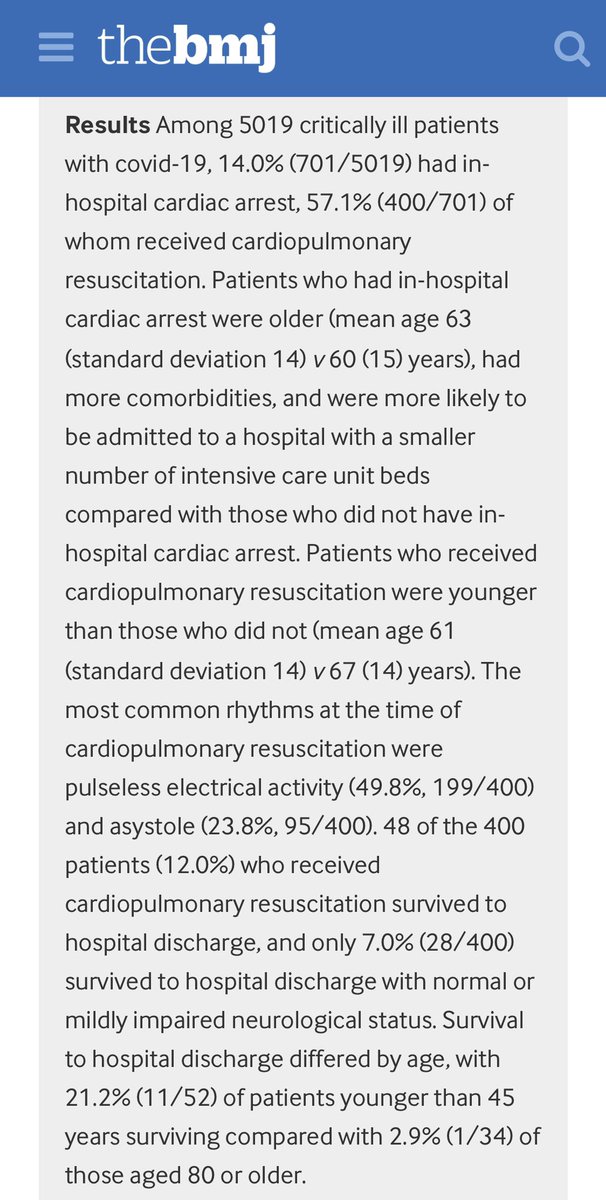
Starting with the British study. bmj.com/content/371/bm…
Starting with the British study. bmj.com/content/371/bm…
First, a mea culpa.
Even though this study is published in the “British Medical Journal”, is is actually a cohort study in *American* hospitals. 🤦♂️
Even though this study is published in the “British Medical Journal”, is is actually a cohort study in *American* hospitals. 🤦♂️

What did they do?
This group followed COVID patients sick enough to be admitted to intensive care units, and asked the following key questions:
1) How many had cardiac arrest?
2) What kinds of did they have?
3) What was done about them?
4) Any key differences?
This group followed COVID patients sick enough to be admitted to intensive care units, and asked the following key questions:
1) How many had cardiac arrest?
2) What kinds of did they have?
3) What was done about them?
4) Any key differences?
A little aside on “cardiac arrest”.
Since we cardiologist (let alone civilians) have been confusing “myocarditis” with any manner of heart condition, we should be sure of what we are talking about.
Since we cardiologist (let alone civilians) have been confusing “myocarditis” with any manner of heart condition, we should be sure of what we are talking about.
For me, I think of “cardiac arrest” as a situation in which there is sudden loss of the ability of the heart to usefully pump blood to the rest of the body.
This is a functional definition, and does not attribute any particular cause.
This is a functional definition, and does not attribute any particular cause.
I will ask a series of polls to make sure we are all on the same page.
What if the heart stops beating completely? Is that cardiac arrest?
What if the heart stops beating completely? Is that cardiac arrest?
Okay, how about if the heart is beating, but in a completely random and uncontrolled manner, such that it is not propelling any blood towards the body?
How about if a huge hole blew out in the side of the heart, and instead of going out the aorta, all of the blood is shooting out the hole and none is going through the aorta?
Wow.
I’m just gonna pause here so I can give a chance for the cardiologists & critical care docs to wake up and start answering these questions. 😏
I’m just gonna pause here so I can give a chance for the cardiologists & critical care docs to wake up and start answering these questions. 😏
• • •
Missing some Tweet in this thread? You can try to
force a refresh