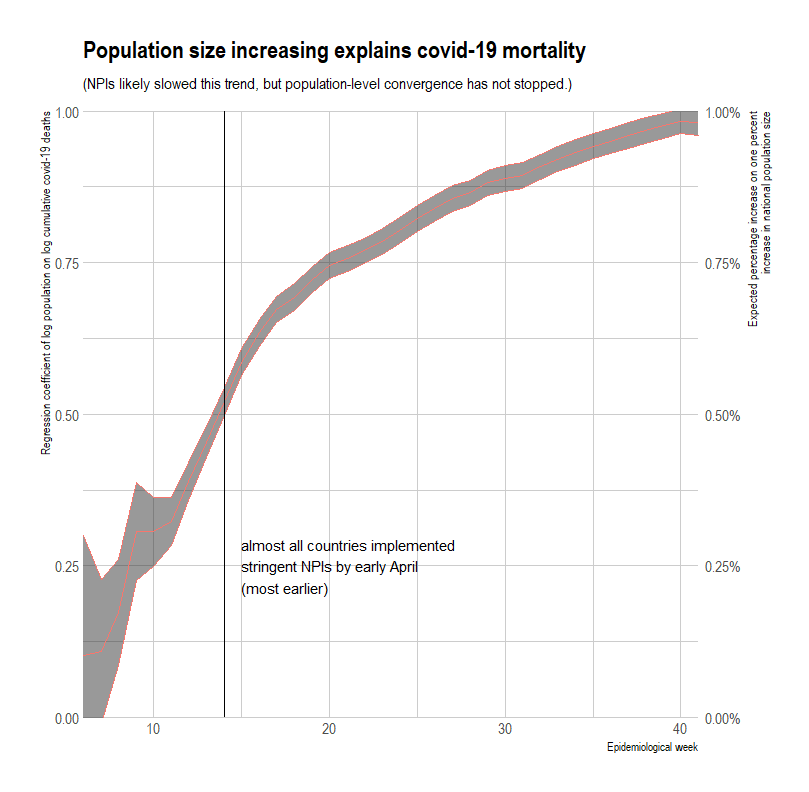
There has been substantial convergence of covid-19 deaths. 

In heatmap form with exponential color steps

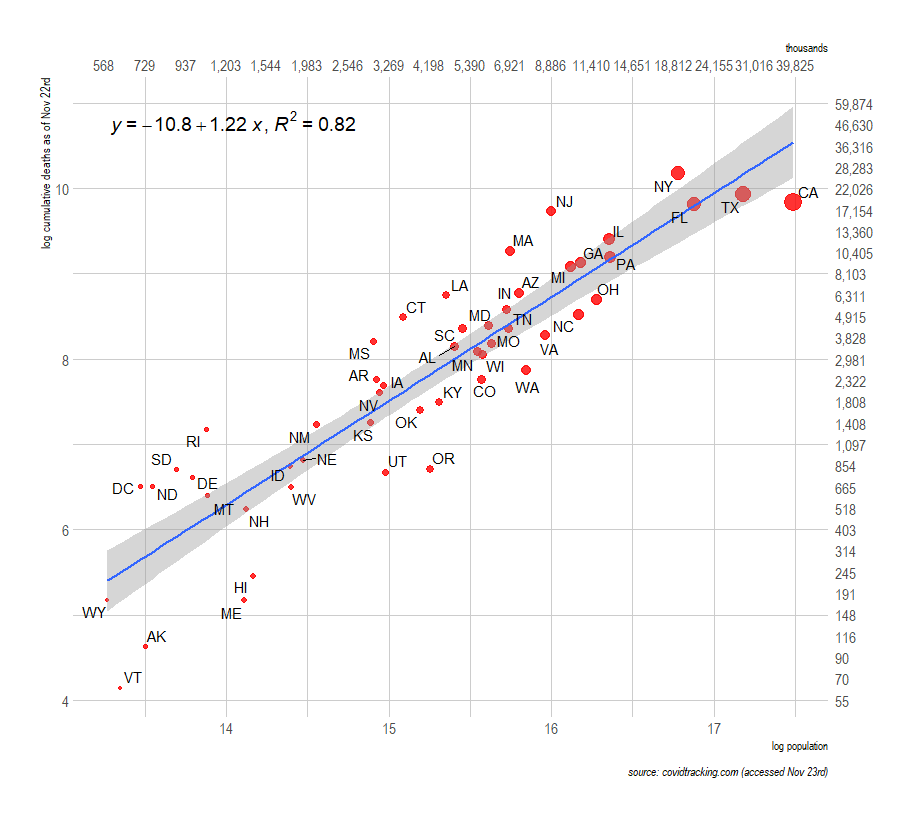
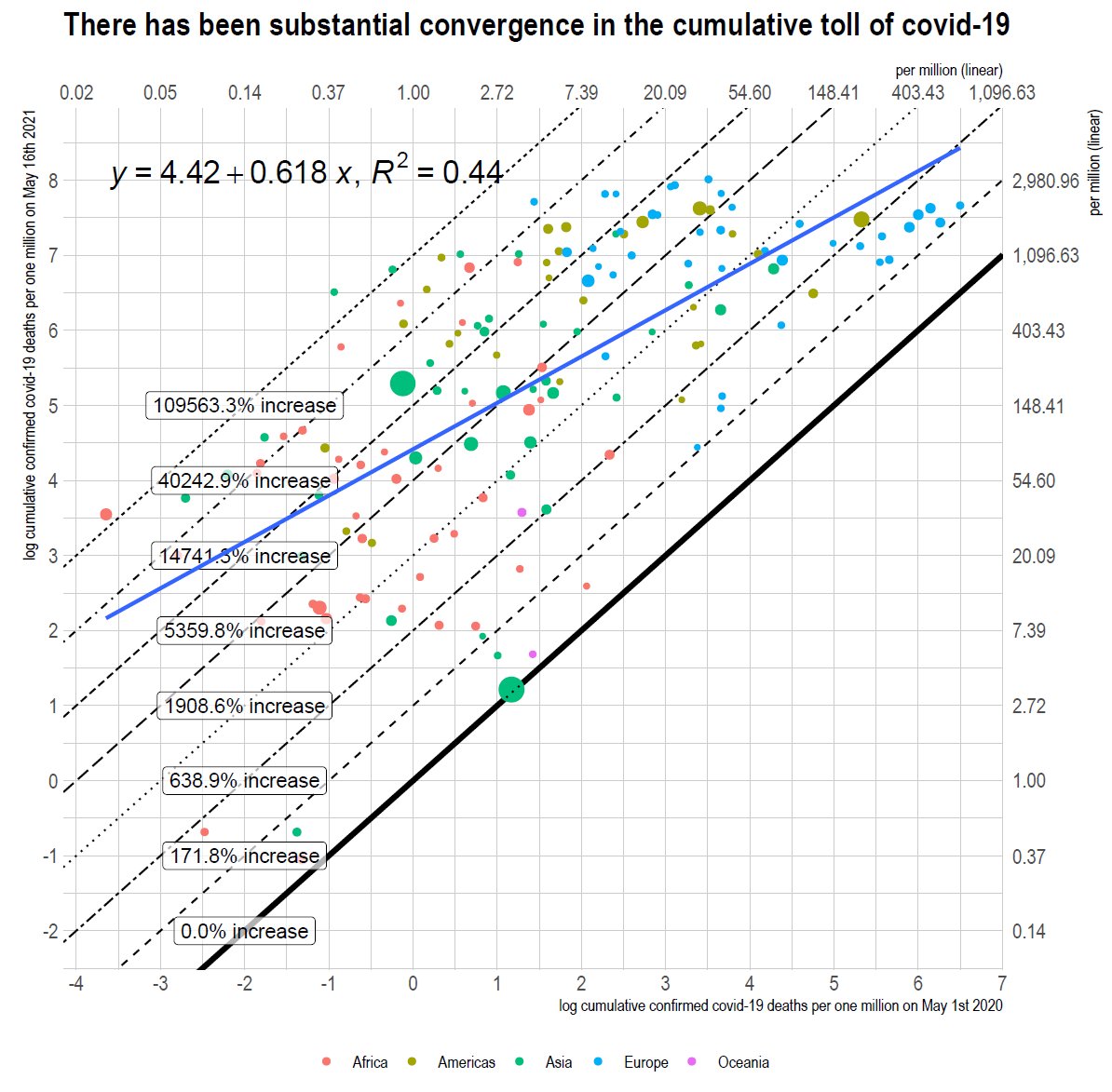
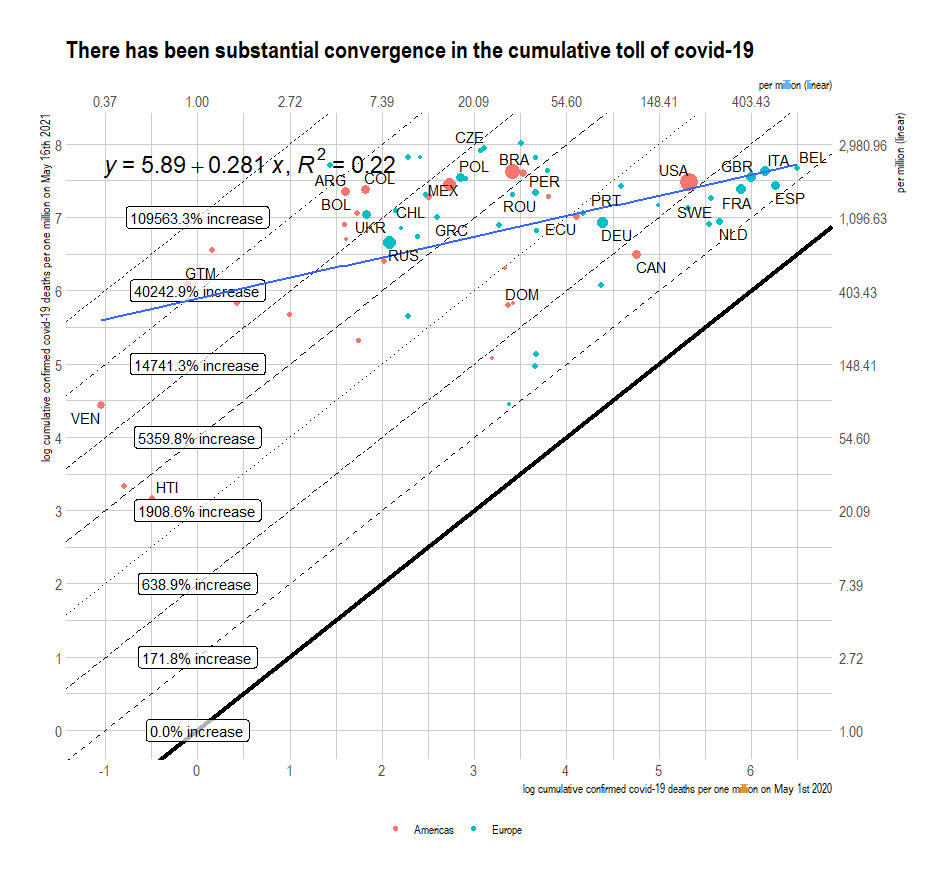
In regression terms
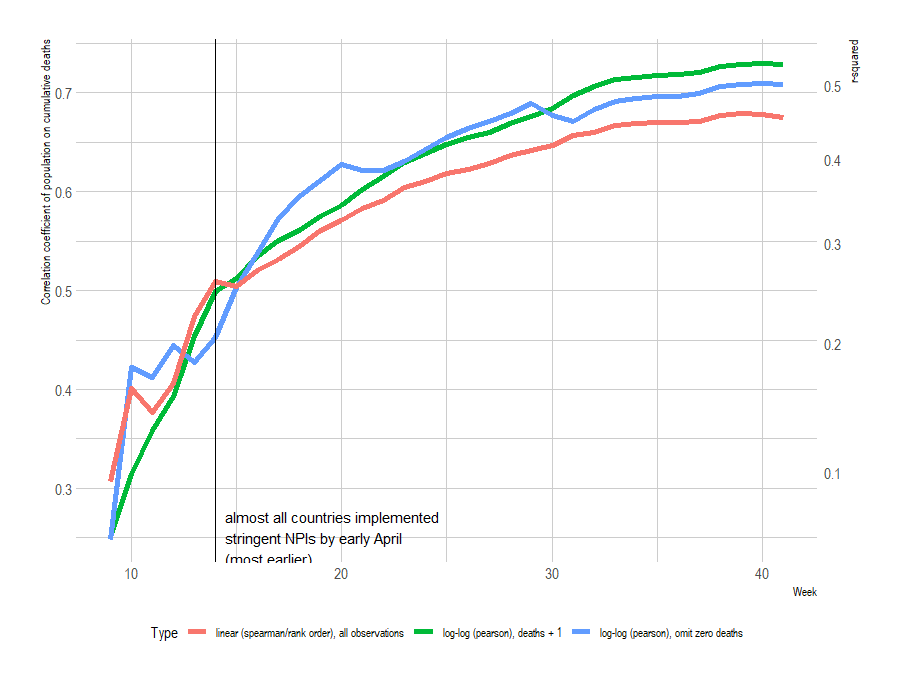
In correlational terms
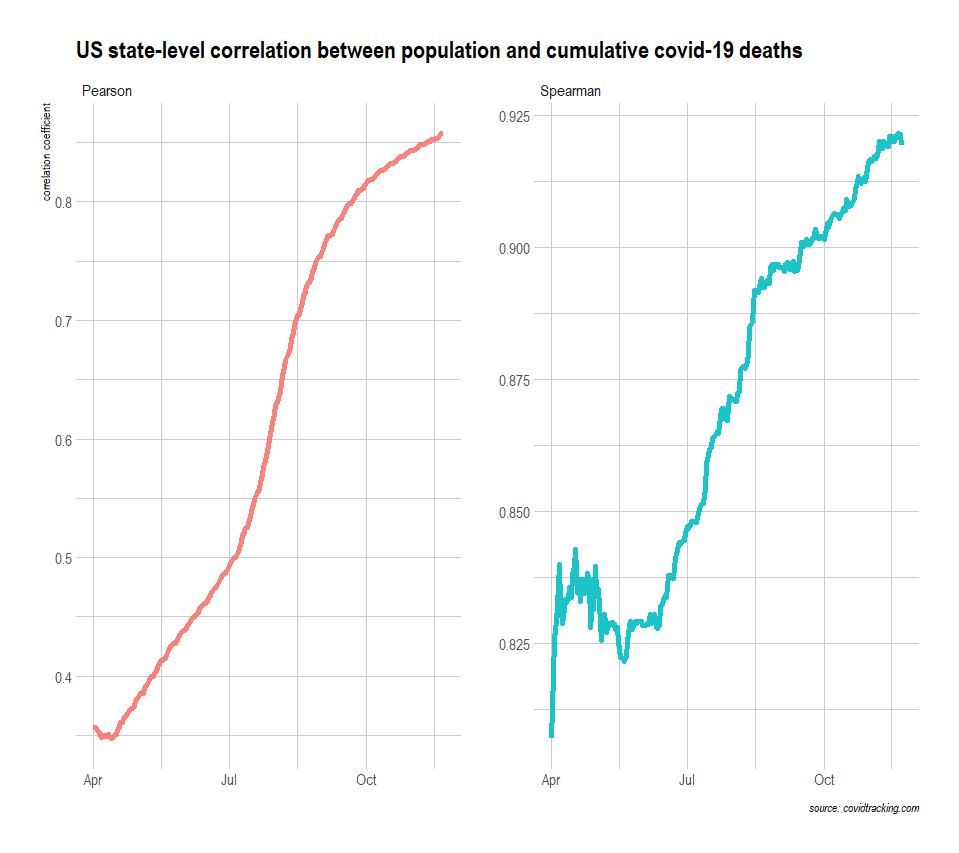
Pearson without log transformation. The initial correlation was negligible since cumulative deaths were very much overdispersed at the outset. Still is, but less and less as time passes.

US state-level correlation between cumulative covid-19 deaths and population
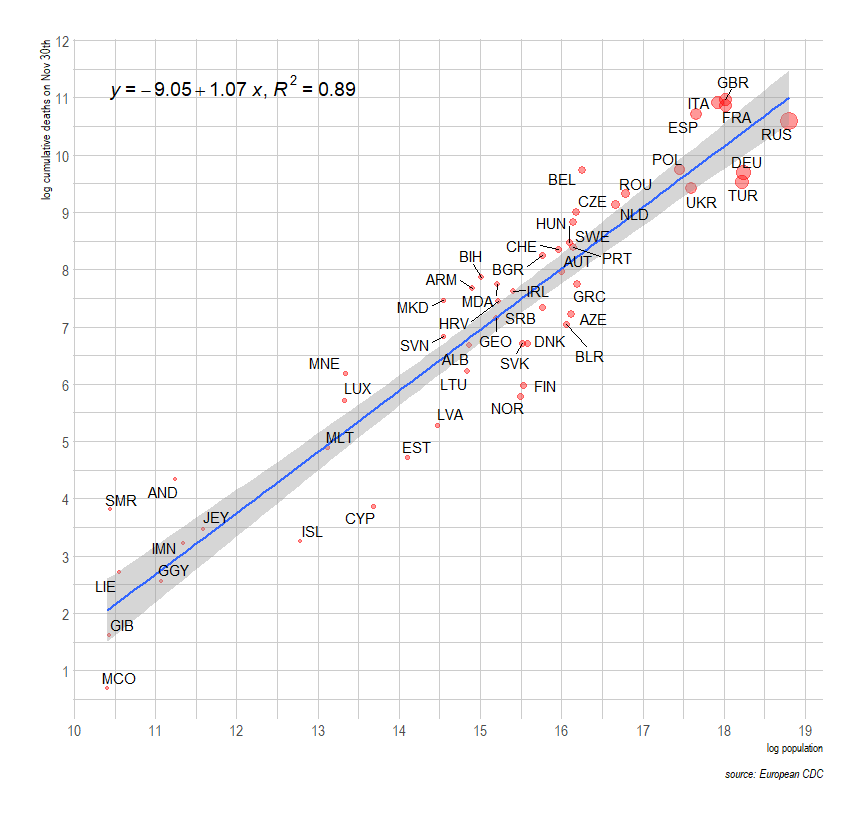
Current cumulative deaths versus population
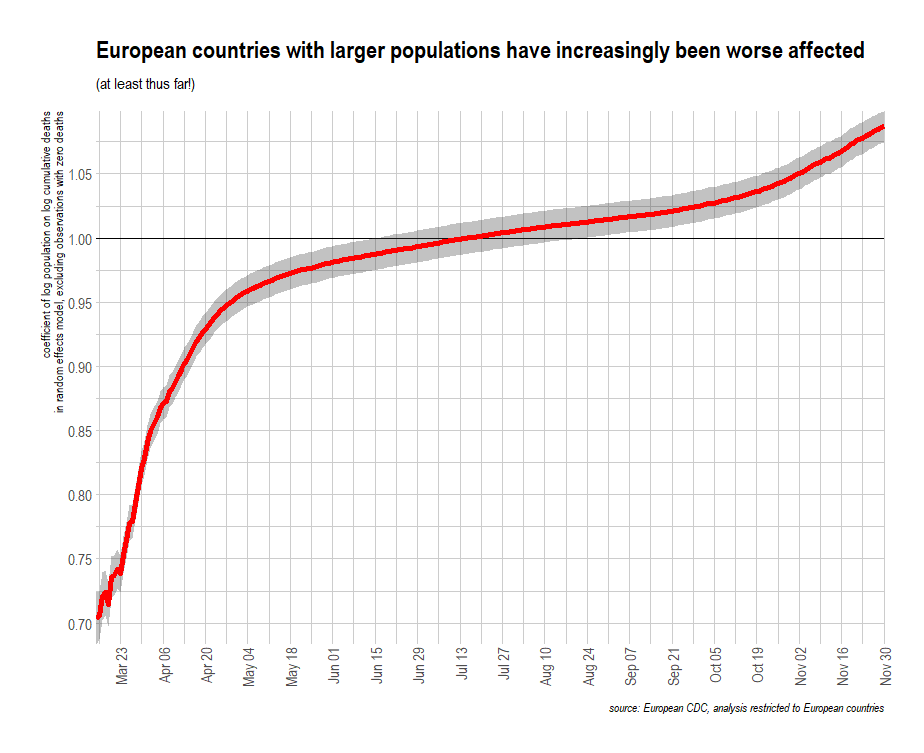
Europe continues to converge vis-a-vis cumulative covid-19 deaths and population.
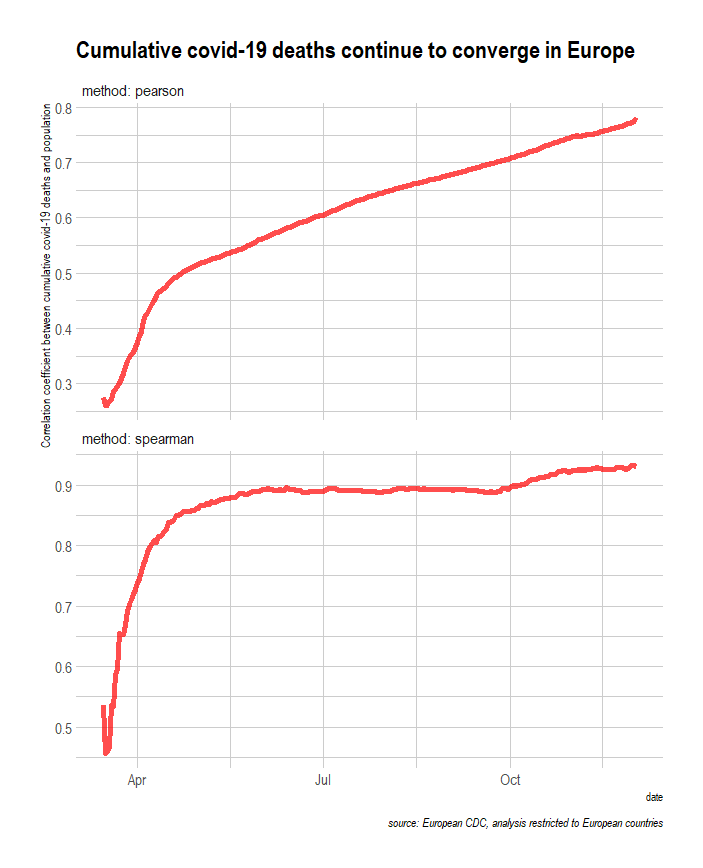
Within Europe, the coefficient of log population on log cumulative deaths crossed unity (>=1) this summer and seems to be trending somewhat higher still.
Most metro areas in the US have converged substantially closer to New York City's cumulative covid-19 deaths on a per capita basis.
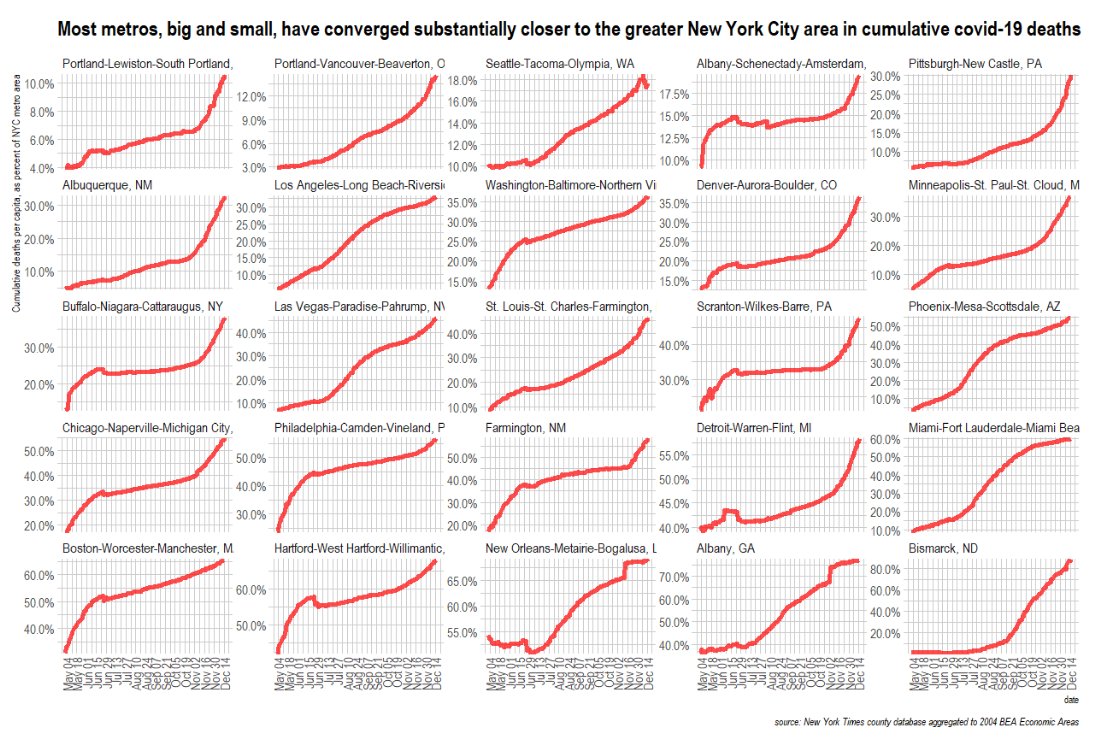
Animated (smaller, more economically peripheral places in the US have substantially converged on the outcomes of larger economies that were generally hit earlier and harder)
Larger populations and economies within the United States and European Union (plus affiliated) affected systematically earlier. Still, there has been substantial subsequent convergence at multiple levels.
Updated and on an entirely per capita basis....
Likewise, but with total GDP (b/c gravity model, tho the coefficient on per capita income clearly significant)
Between May 1st of last year and today, pretty much all countries saw large increases in cumulative covid-19 mortality, with initially less affected countries experiencing more growth (esp. within Europe and the Americas)
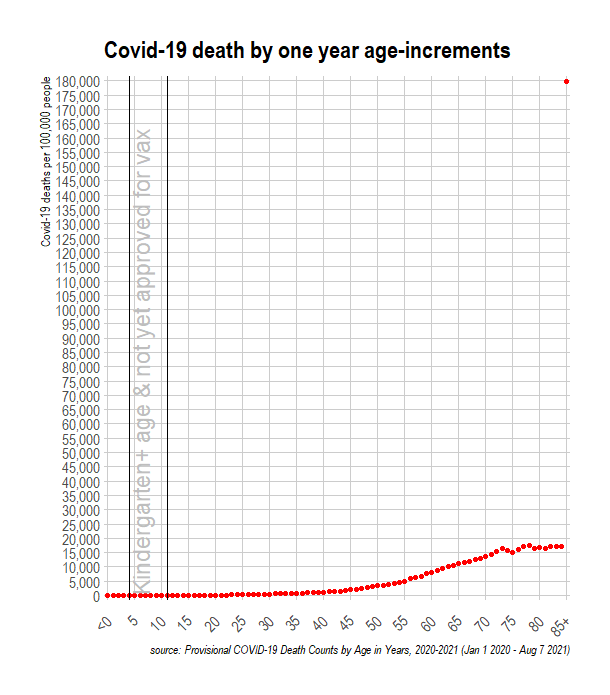
The convergence process is surely more pronounced in age-conditional terms, as it hit larger, higher-income economies first, which skew quite a bit older.
(Never mind the issues with accurately detecting and reporting covid deaths as covid deaths and other factors like climate....)
Same plot, but just for the Americas and Europe
• • •
Missing some Tweet in this thread? You can try to
force a refresh