
So many great ID 💎💎💎 with @dsolsMD at morning report today, discussing a case of preseptal cellulitis + parotitis!
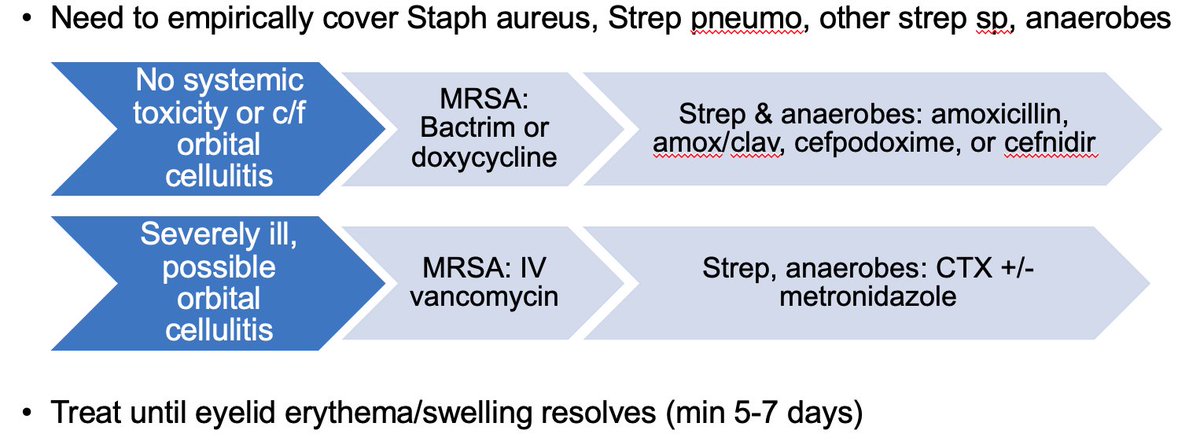
🦠Staph aureus, Strep sp, and anaerobes 🦠 implicated!
Preseptal cellulitis - infection anterior to orbital septum - can be differentiated from orbital cellulitis by pain with EOM 👀🙄 due to inflammation of extra ocular muscles and fatty tissue.
Preseptal cellulitis - infection anterior to orbital septum - can be differentiated from orbital cellulitis by pain with EOM 👀🙄 due to inflammation of extra ocular muscles and fatty tissue.


When contemplating 💊:
1. who is the host? Not as simple as immunocompromised 😷 or not. Consider "area under curve" - total lifetime exposure to immune suppressing medications or conditions.
1. who is the host? Not as simple as immunocompromised 😷 or not. Consider "area under curve" - total lifetime exposure to immune suppressing medications or conditions.
2. Are you worried about MRSA? Community acquired MRSA on decline, but rate as high as ~30%. If orbital cellulitis is on ddx, make sure to cover!
A few pro tips:
💎 When switching from IV to PO, pick 💊 with higher PO bioavailability - linezolid, fluoroquinolones, bactrim, doxycycline, metronidazole, fluconazole (not cephalosporins, PCNs)
💎 Thinking cephalexin? Use cefadroxil instead - BID > QID!
💎 When switching from IV to PO, pick 💊 with higher PO bioavailability - linezolid, fluoroquinolones, bactrim, doxycycline, metronidazole, fluconazole (not cephalosporins, PCNs)
💎 Thinking cephalexin? Use cefadroxil instead - BID > QID!
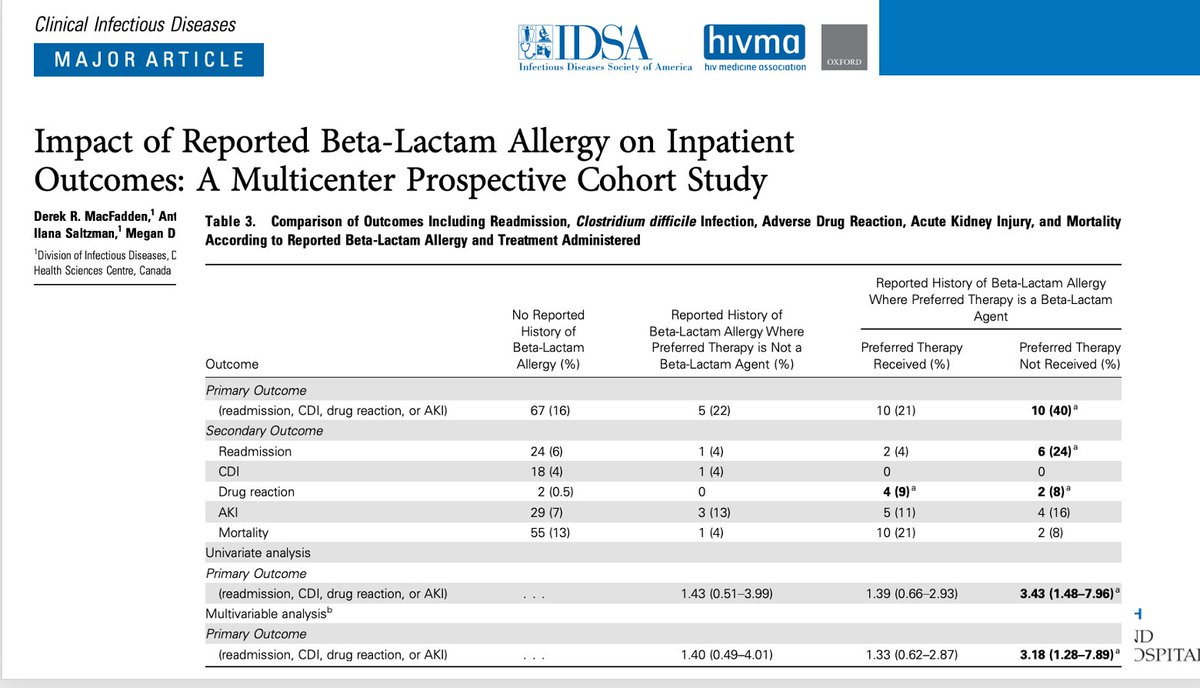
Beta lactam allergy in chart? Collect a careful allergy history & weigh risks of undertreated infection vs. risk of allergic reaction. Study in CID shows ⬆️ readmission and medication side effect if given 2nd line non beta lactam therapy due to reported allergy.
• • •
Missing some Tweet in this thread? You can try to
force a refresh










