
More important findings from the newly uncovered RI PCR test Ct data!
Recall I previously showed the Ct values of more than 5000 C19 PCR tests from the RI state health lab. Here they are again color coded for estimated infectivity. While all these folks were “positive”...
Recall I previously showed the Ct values of more than 5000 C19 PCR tests from the RI state health lab. Here they are again color coded for estimated infectivity. While all these folks were “positive”...
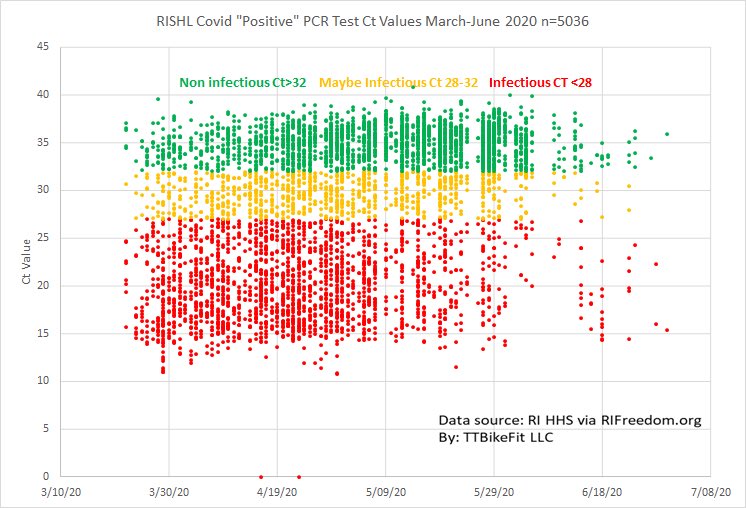
The green folks were likely not infective and the yellows may not have been. The higher the Ct score, the lower the viral load - the person is “less sick” or has remnant viral rna which can be detected for months while infectivity lasts maybe a week.
Yet it is nearly impossible to obtain Ct score data! Go ahead and ask for it- you will likely get a blank stare or a weak excuse about authorization or data storage. But you won’t get your Ct score. Ridiculous.
Now look what happens if we take the mean Ct values for each day- a clear trend emerges. As we moved into May the means climbed over 30. The average person receiving a positive test result was likely not infectious! What I believe @MichaelYeadon3 has termed a “cold positive”

The plot thickens when we add daily fatalities (7d ma). Here I have offset them by 21 days. The appropriate lag from test to fatality is arguable, but the point is as Ct values increase (avg viral load decreases), fatalities 3 weeks later decrease. Significantly...
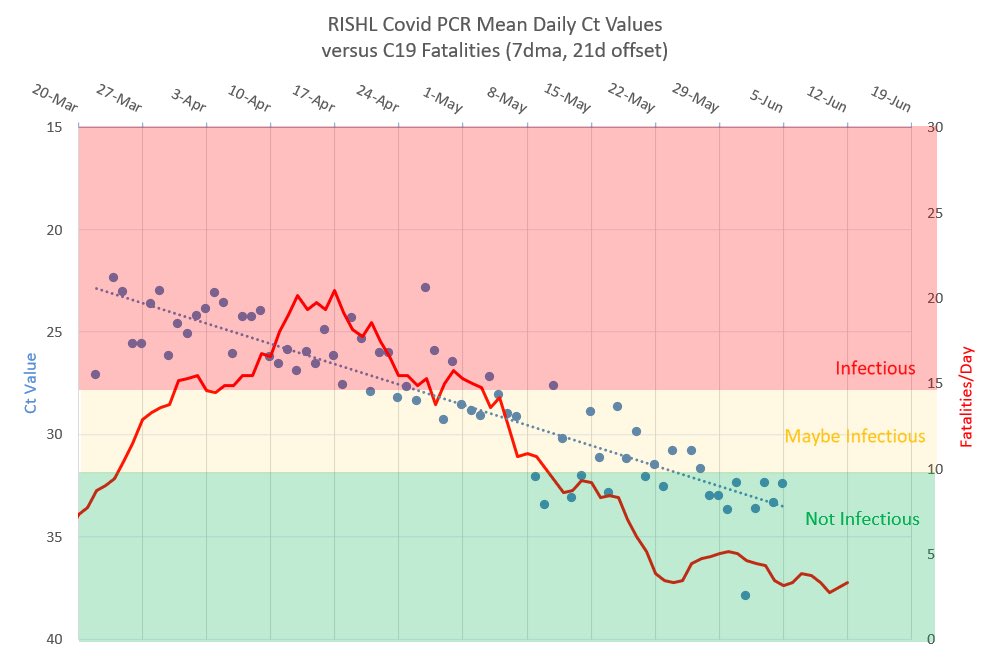
As the average Ct rises past 30, deaths almost disappear.
Seems like reporting and tracking of Ct values would be very important for tracking the severity and progress of the pandemic! Trends in Ct PREDICT severity - and why wouldn’t they as Ct tracks viral load!
Seems like reporting and tracking of Ct values would be very important for tracking the severity and progress of the pandemic! Trends in Ct PREDICT severity - and why wouldn’t they as Ct tracks viral load!
Yet we only receive a binary yes/no test result. PCR testing w/o Ct tracking is a blunt instrument used to bludgeon us into compliance and create a casedemic while the very important insights Ct scores could provide is ignored by “public health experts.” This must change!
Thanks again to @andrewbostom for suppling the data; uncovered via a FOIA request by RIFreedom.org
And now this comes to light- after 9mos the WHO recommends (in a wishy washy way) that Ct should be lowered and pcr can be prone to false positives. 🤔
https://twitter.com/emmakennytv/status/1339347790766477318?s=21https://t.co/AoiFSNFrck
• • •
Missing some Tweet in this thread? You can try to
force a refresh












