Sir Mansel Aylward talks about his experience of #LongCovid
bbc.co.uk/news/uk-wales-…
bbc.co.uk/news/uk-wales-…
I hope his reflections go slightly deeper than just the UK's unpreparedness... meassociation.org.uk/2011/11/privat…
Further reading from @TommyShakes | Blaming the victim, all over again: Waddell and Aylward's biopsychosocial (BPS) model of disability
journals.sagepub.com/doi/abs/10.117…
journals.sagepub.com/doi/abs/10.117…
More further reading: Getting rich on disability denial @RedPeppermag redpepper.org.uk/getting-rich-o…
Psychological tyranny prescribed by the DWP: preventable harm is government policy | B J Gen Pract 2018
ncbi.nlm.nih.gov/pmc/articles/P…
ncbi.nlm.nih.gov/pmc/articles/P…
Who is Prof Sir Mansel Aylward? lshubwales.com/board/professo…
Problems in the assessment of psychosomatic conditions in Social Security benefits and related commercial schemes | J Psychosom Res 1995 pubmed.ncbi.nlm.nih.gov/8568732/
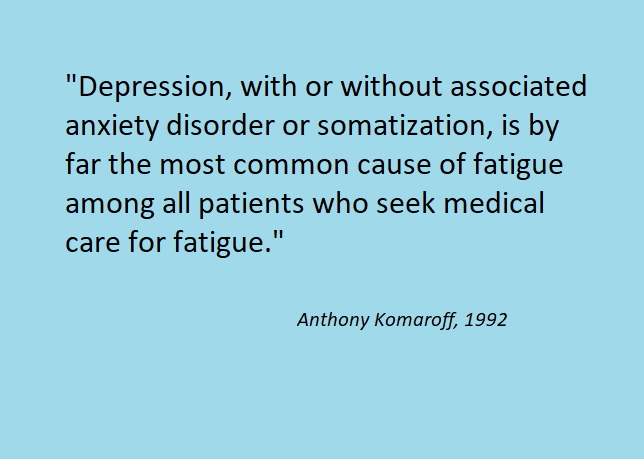
"Some diagnoses are purely subjective by definition..." 

Models of sickness and disability | Waddell and Aylward 2010 webility.md/praxis/downloa…
Who was Gordon Waddell journals.lww.com/pain/Citation/…
Part of the problem is the assumption that such a "medical model" actually exists.

When actually this seems to be a description of one of a number of different scenarios, where the ideal "model" is at the top.

Another big assumption about the "medical model" is that it makes assumptions.

From my own experience, application of BPS in healthcare, rather than addressing complex issues in a multifactorial way, essentially reduces it to "guided self-help", and further exacerbates the problem.
Dog whistle medicine and disability denial - Unum, Aylward and the "Wessely School"
https://x.com/newhealthpsych/status/1375085863818952708
Aylward also contributed a section to the Trends in Health and Disability 2002 report (Unum) - it's quite dry though. The section by a certain Dr Sharpe is more interesting... web.archive.org/web/2003012615…
"Both State and private insurers pay people to remain ill."
Nice dig at patient support groups and charities there too. 😠
Nice dig at patient support groups and charities there too. 😠

No mate, biggest obstacle to recovery is lack of effective treatments.

Sharpe mentions the 2002 CMO report, which I linked to here:
https://x.com/_Lucibee/status/1372869367512363012
"Neither classification [DSM-IV vs ICD-10] is ideal."
aka "We're not saying that it's psychological... (but it's psychological.)"
aka "We're not saying that it's psychological... (but it's psychological.)"

"The trial was co-designed with a patient group."
https://x.com/zaranosaur/status/1376219252810735622

Another clipping to append to this thread...
https://x.com/maxwhd/status/1378406787498582017
@threadreaderapp please unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh