LISTEN as highly influential Prof John Conly (upper left) of UCalgary, AHS CV19 sci advisory grp, Public Health Agency Canada, Chair WHO Infection Prevention & Control R&D Expert Grp. opposes N95 wearing citing acne harm vs @DFisman & @kprather88 precautionary principle. /1
"there's been decreased O2 concentrations in pregnant women" yeah, well here's the reference from one of his publications, dissected in fine form by @caruzycki /2
https://twitter.com/caruzycki/status/1380711275307540481?s=20
Here's an example of Prof Conly's influence by the dedicated @jmcrookston /3
https://twitter.com/jmcrookston/status/1316441457675431936?s=20
What would a dermatologist prefer, acne or COVID-19? Let's find out! /4
https://twitter.com/lisa_iannattone/status/1380596564910047240?s=20
Because of Prof. Conly's influence, public health agencies around the world continue to double down on contact and droplet. Public Health Ontario: /5 
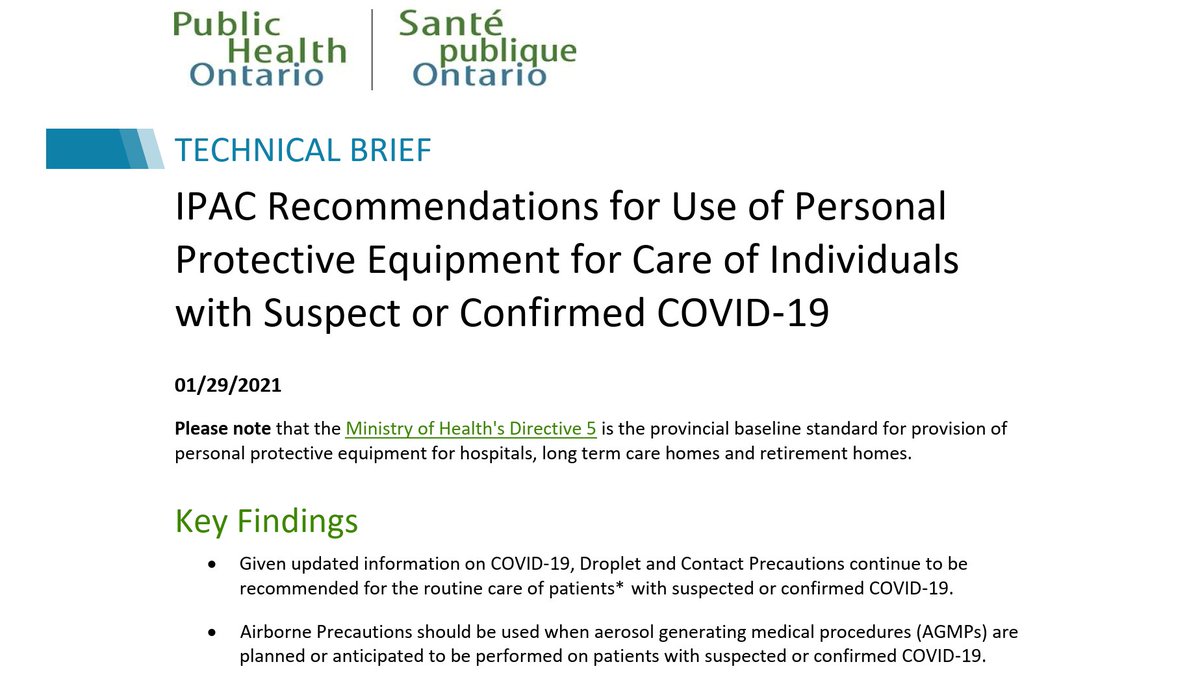
February 19, 2021 Directive 5 FAQ from Ontario Ministry of Health & LTC:
Droplet & Contact precautions, and conserve PPE.
Conserve PPE, despite ample supplies. One year into the pandemic. It's egregious. /6
Droplet & Contact precautions, and conserve PPE.
Conserve PPE, despite ample supplies. One year into the pandemic. It's egregious. /6

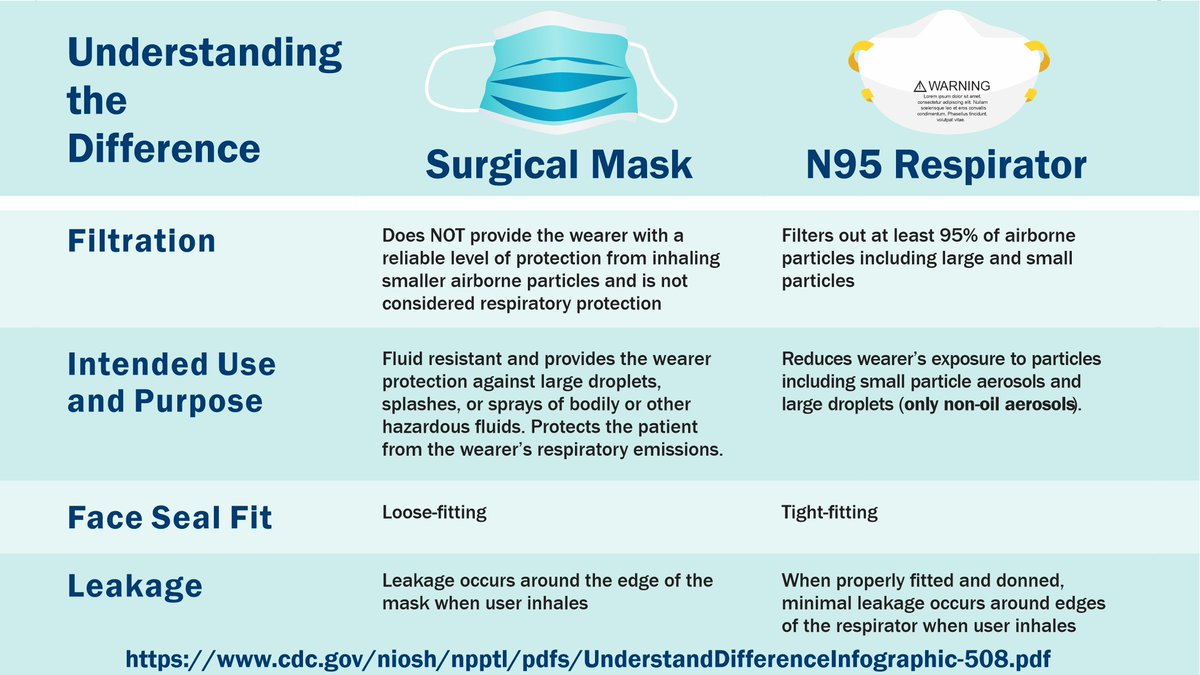
Here's what the CDC and NIOSH have to say about the differences between Surgical Masks and N95 Respirators. /7
(image adapted from ) cdc.gov/niosh/npptl/pd…
(image adapted from ) cdc.gov/niosh/npptl/pd…
The presentations by Prather and Fisman make an excellent summary of how the wide variance in respiratory aerosols produced by people can explain the high dispersion factor of COVID-19. Highly recommended to view the 60 minute session in its entirety /8 ucalgary.yuja.com/V/Video?v=3323…
Dr. Conly is the primary & corresponding author of WHO commentary article stating "SARS-CoV-2 not airborne to any significant extent, respirators offer no advantage & may result in unintended harms" same as he said in the video above /9 aricjournal.biomedcentral.com/articles/10.11…

Regarding the poor experimental design leading Conly to claim N95 leads to "decreased O2 concentrations in pregnant women", thread is archived here:
OF COURSE you can't get much air when you're breathing through such a restricted contraption. /10
OF COURSE you can't get much air when you're breathing through such a restricted contraption. /10
https://web.archive.org/web/20210509022537/https://twitter.com/caruzycki/status/1380711275307540481

• • •
Missing some Tweet in this thread? You can try to
force a refresh

![States high levels of CO2 and other contaminants ... can contribute to [list of five health effects, such as headaches, fatigue, difficultly concentrating], says CO2 should be below 1000 ppm, then says (incorrectly) that health effects from CO2 occur at levels above 5000 ppm. No, those effects can occur below 5000 ppm. It also states the CO2 concentrations do not indicate a risk of infectious disease transmission in a space. No, ASHRAE's position statement on CO2 states that elevated CO2 concentrations CAN reflect higher risk. Obviously, because it indicates poor ventilation, which IS an i...](https://pbs.twimg.com/media/GO6z_36WQAI7_mj.jpg)