
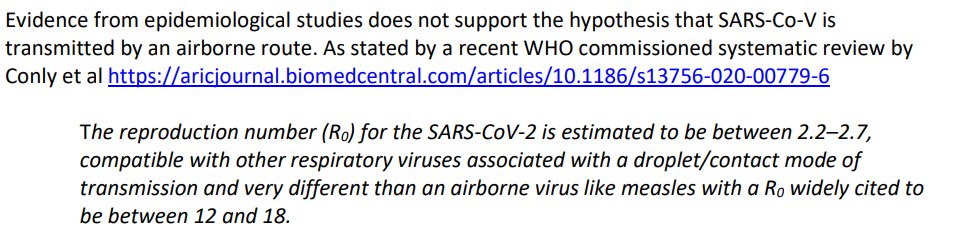
On the airborne argument, fundamentally the reason they won't agree to ever change. 

From UK IPS

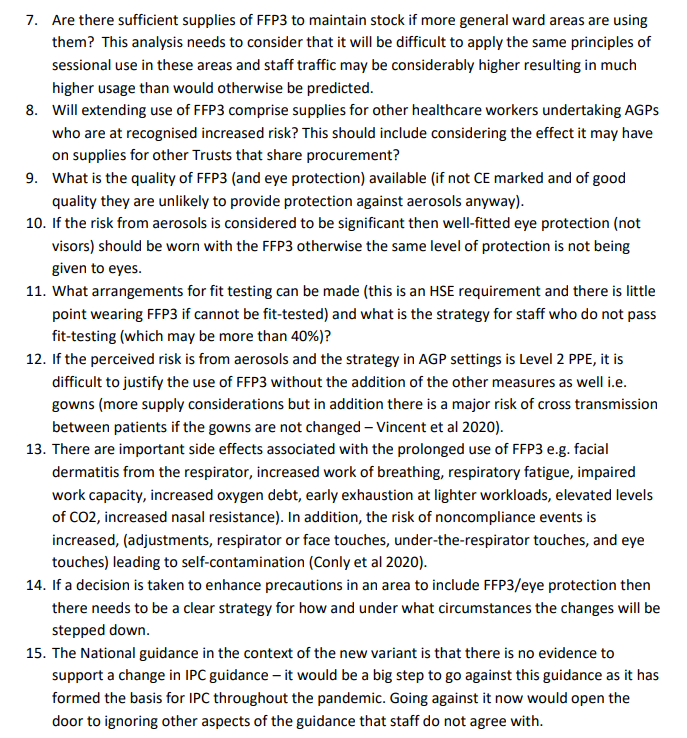
Note the concern with breaking ranks from national guidance, which of course would apply similarly at national up to international level.
That's not the most fun you can have with that document.
File name is Healthcare-workers-and-FFP3-Version-2.1-27-01-21.pdf for anyone who wants to find it online.
Not true/excuses...

Hmm name is familiar...
People know exactly why ICU is lower (they wear masks, patients less infective by then) and why it's higher for admin/etc staff (no masks, but exposed to COVID-19).

Admitted later in same doc
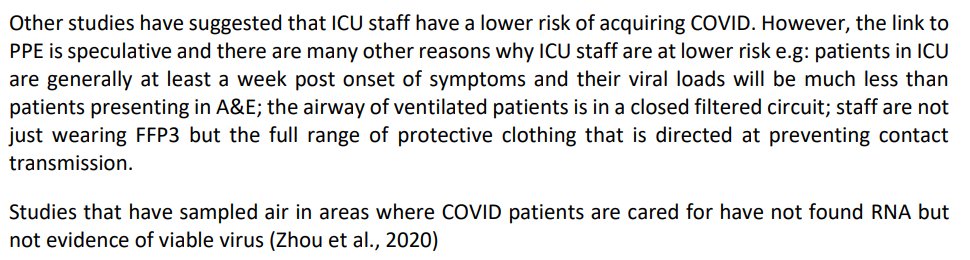
No viable virus = old excuse come up with new ones already.
Social distancing blame in a hospital? Or, give em masks. But hey we're not here to stop spread are we?
Social distancing blame in a hospital? Or, give em masks. But hey we're not here to stop spread are we?

That name again ...

Same Loeb as is running an RCT on masks right now.
Hrm, geniuses at work here.
Hrm, geniuses at work here.

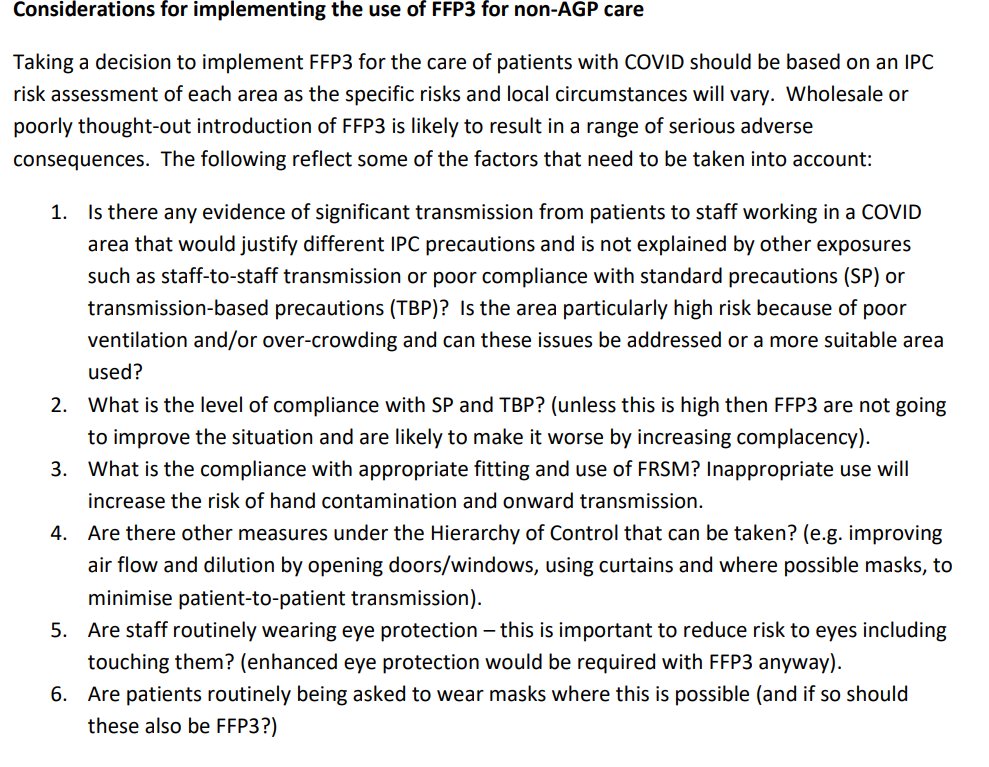
In what is for IPC, even for them, a huge reach (although maybe not as much a reach as for rats spreading SARS), they argue don't bother with masks because
MASKS DO NOT COVER YOUR EYES
(so why bother w the mask anyway, I guess is how that argument must end)
MASKS DO NOT COVER YOUR EYES
(so why bother w the mask anyway, I guess is how that argument must end)

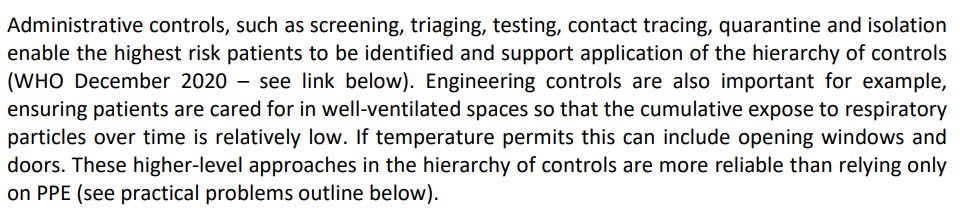
Also inconsistent: ventilate the hell out of the space to reduce particles in the air, but don't give them masks.
What?
So, only in rooms with AGMPs do you wear masks? But you should ventilate everywhere? Because stuff floats? But NOT wear masks? But what? But I'm dizzy now.
What?
So, only in rooms with AGMPs do you wear masks? But you should ventilate everywhere? Because stuff floats? But NOT wear masks? But what? But I'm dizzy now.
HEY DONT TOUCH THAT MASK until you have performed this
492 step process
and assessed
all the risks
because that's FIFTY CENTS RIGHT THERE BUDDY
492 step process
and assessed
all the risks
because that's FIFTY CENTS RIGHT THERE BUDDY
• • •
Missing some Tweet in this thread? You can try to
force a refresh





