A thread on what studying "AGPs" tells us about 'aerosols and droplets'
Focus on this paper
…-publications.onlinelibrary.wiley.com/doi/10.1111/an…
Done in Sydney
Hats off to @NWilson247 @EuanTovey
My role was microscopic
First: discussion should be 'what is the proportion of each in disease risk: not A vs B
Focus on this paper
…-publications.onlinelibrary.wiley.com/doi/10.1111/an…
Done in Sydney
Hats off to @NWilson247 @EuanTovey
My role was microscopic
First: discussion should be 'what is the proportion of each in disease risk: not A vs B
The study builds on work by others esp Bristol AERATOR study which has examined designated 'aerosol generating procedures' in a laminar flow theatre
-intubation/extubation
-NIV/HFNO
-tracheostomy
& largely identified a LACK of aerosol
More to come on other designated AGPs
-intubation/extubation
-NIV/HFNO
-tracheostomy
& largely identified a LACK of aerosol
More to come on other designated AGPs



AERATOR papers
…-publications.onlinelibrary.wiley.com/doi/epdf/10.11…
journals.sagepub.com/doi/full/10.11…
medrxiv.org/content/10.110…
…-publications.onlinelibrary.wiley.com/doi/epdf/10.11…
journals.sagepub.com/doi/full/10.11…
medrxiv.org/content/10.110…
For balance here are some studies with slightly different conclusions
ccr.cicm.org.au/config/cicm-cc…
…-publications.onlinelibrary.wiley.com/doi/full/10.11…
ccr.cicm.org.au/config/cicm-cc…
…-publications.onlinelibrary.wiley.com/doi/full/10.11…


Another important paper by @nate_gaeckle
Studied NIV/HFNO in a clean isolation chamber
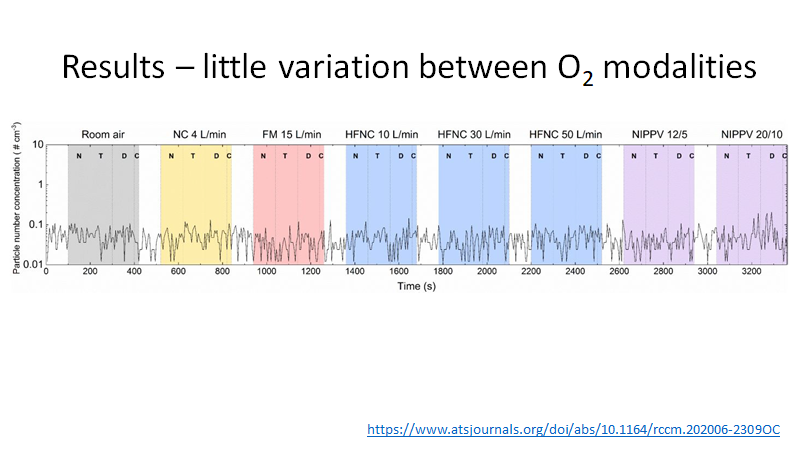
showed
-no more aerosol than other oxygen delivery methods
-massive variation between individuals
atsjournals.org/doi/full/10.11…
Studied NIV/HFNO in a clean isolation chamber
showed
-no more aerosol than other oxygen delivery methods
-massive variation between individuals
atsjournals.org/doi/full/10.11…
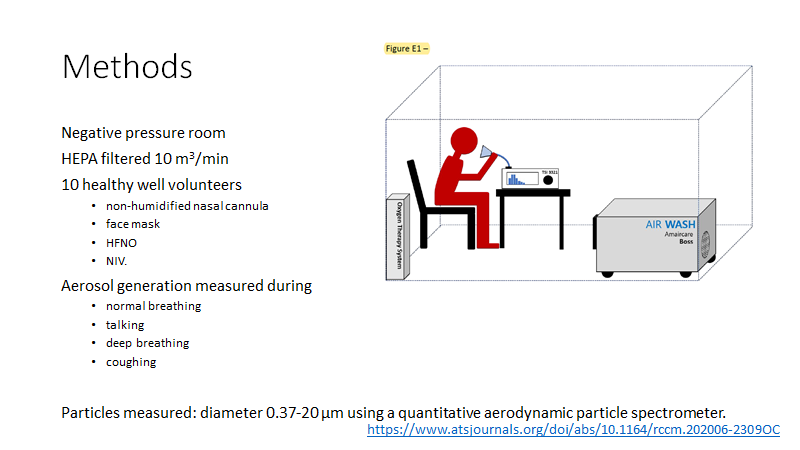


Key in all these studies is conduct in ULTRAclean (HEPA filtered) environment
...needed to detect respiratory aerosols (signal) over non-respiratory (noise)
Note
-noise amplitude >> signal
-size distribution differs
(studies in non-clean settings can be ignored!)
...needed to detect respiratory aerosols (signal) over non-respiratory (noise)
Note
-noise amplitude >> signal
-size distribution differs
(studies in non-clean settings can be ignored!)

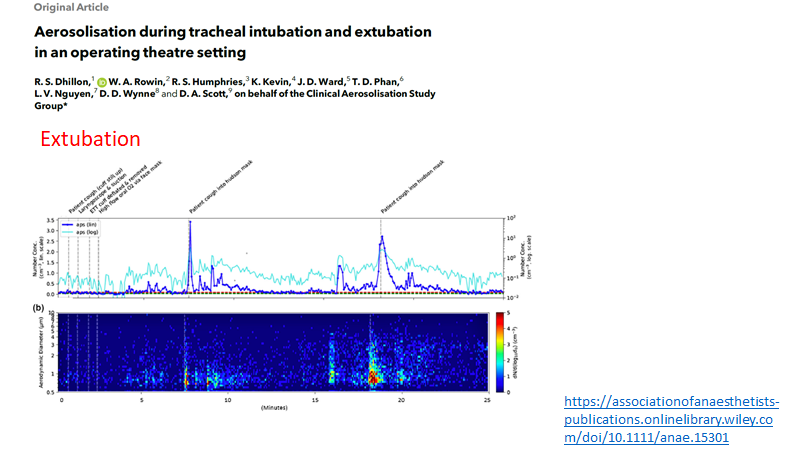
...back to the paper at hand
…-publications.onlinelibrary.wiley.com/doi/10.1111/an…
Done in an ultraclean chamber
Key difference from other papers
-massive head sized cone
-high sampling rates
to try to capture ALL exhaled aerosol
…-publications.onlinelibrary.wiley.com/doi/10.1111/an…
Done in an ultraclean chamber
Key difference from other papers
-massive head sized cone
-high sampling rates
to try to capture ALL exhaled aerosol


Expired particles sampled
During respiratory ACTIVITIES
-breathing
-shouting
-exercise
-force expiration
-cough
With respiratory PROCEDURES
-nothing
-NIV or CPAP
-HFNO
-surgical mask
During respiratory ACTIVITIES
-breathing
-shouting
-exercise
-force expiration
-cough
With respiratory PROCEDURES
-nothing
-NIV or CPAP
-HFNO
-surgical mask

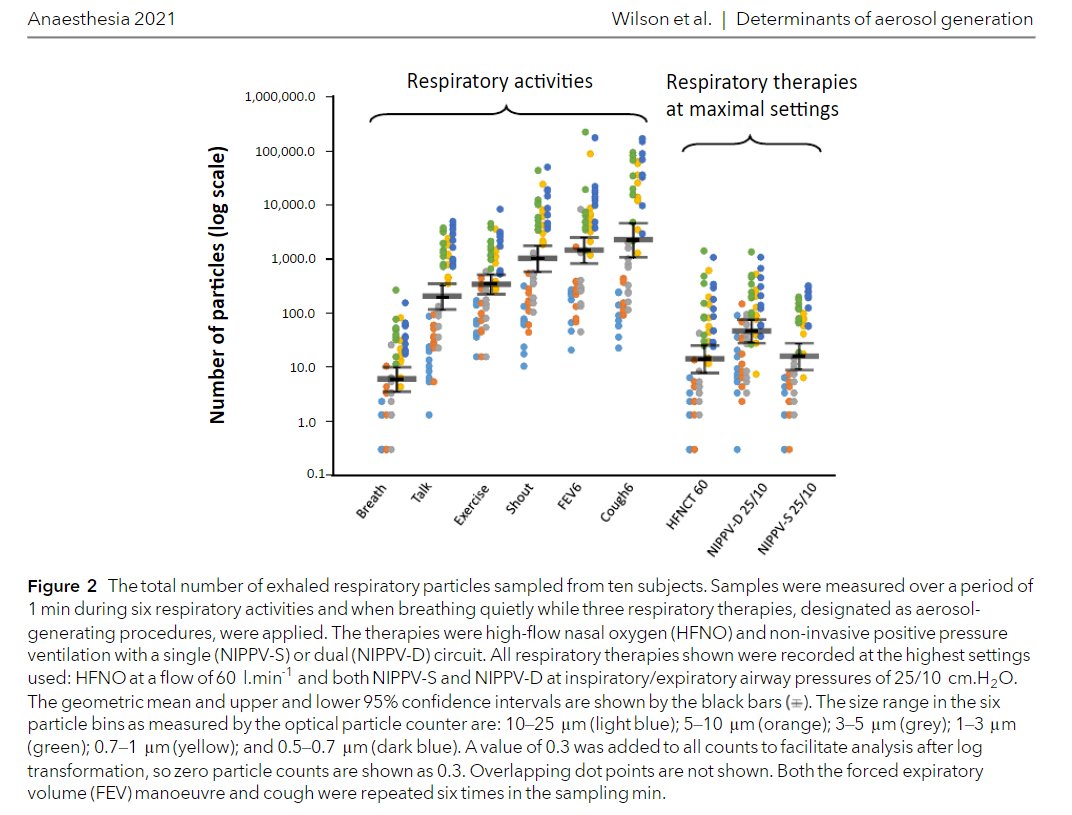
First key finding.
A modest increase in aerosols with respiratory THERAPIES during quiet breathing
BUT (big but) this disappeared & emissions fell with respiratory therapy during exertional respiratory activities
A modest increase in aerosols with respiratory THERAPIES during quiet breathing
BUT (big but) this disappeared & emissions fell with respiratory therapy during exertional respiratory activities


This fall in exhaled aerosols with NIV/CPAP/HFNO compared to without their use shows they are NOT AGPs
The fall likely due to
-PEEP reducing airway collapse and open/close cycling
-positive inward flow reducing egress
The fall likely due to
-PEEP reducing airway collapse and open/close cycling
-positive inward flow reducing egress

You may have picked it up already....
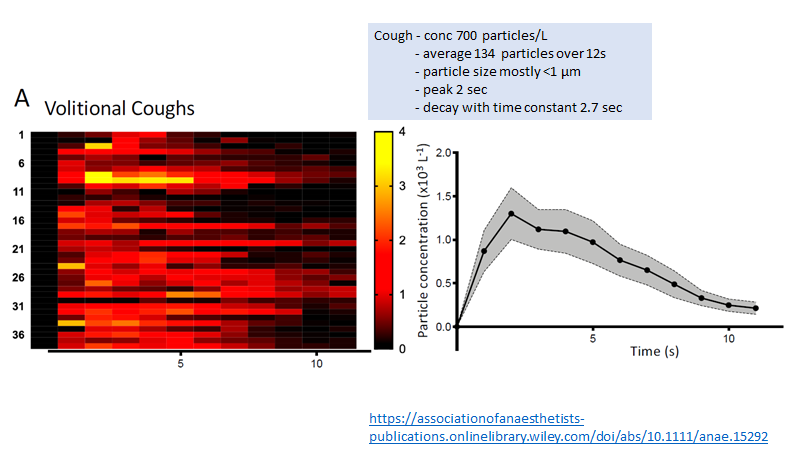
Yes coughing, exercise & forced expiration (each mimicking breathing patterns in illness) produce many-fold more aerosols than quiet breathing (log scale)
Respiratory ACTIVITY should be focus of concern
NOT respiratory PROCEDURES
Yes coughing, exercise & forced expiration (each mimicking breathing patterns in illness) produce many-fold more aerosols than quiet breathing (log scale)
Respiratory ACTIVITY should be focus of concern
NOT respiratory PROCEDURES

For those who want to dive deep here are the particle size distributions (generally >95% <5micron) & the % of all particle volume in these small aerosols
…-publications.onlinelibrary.wiley.com/action/downloa…
…-publications.onlinelibrary.wiley.com/action/downloa…

Again - as per Gaeckle and others - there was a massive inter-individual variation

So what do we learn
1 NIV, CPAP, HFNO are not AGPs
2 Exertional activities (cough, fast deep breathing) generate up to 370-fold more aerosol than quiet breathing
3 This aerosol is respirable
4 It constitutes a significant volume of all expired volume
5 We need to rethink risk
1 NIV, CPAP, HFNO are not AGPs
2 Exertional activities (cough, fast deep breathing) generate up to 370-fold more aerosol than quiet breathing
3 This aerosol is respirable
4 It constitutes a significant volume of all expired volume
5 We need to rethink risk
We know some superspreader events create massive infection & can only be explained by aerosols
These likely combination of
-high viral load (disease time course)
-high risk person (high emitter/spreader)
-high risk activity (sing, shout etc)
-poor ventilation
-prolonged exposure
These likely combination of
-high viral load (disease time course)
-high risk person (high emitter/spreader)
-high risk activity (sing, shout etc)
-poor ventilation
-prolonged exposure
While droplets may be a high risk at short distance...
...the high production of respirable aerosols by exertional respiratory activities (common in illness) point to a prominent role of aerosol transmission at short distances
(& in some settings over long distances)
...the high production of respirable aerosols by exertional respiratory activities (common in illness) point to a prominent role of aerosol transmission at short distances
(& in some settings over long distances)
The other point I should’ve made. Even more important than an ultraclean setting..
....collaboration between aerosol/environment scientists & clinicians
Key to all the papers in the thread (& missing from many others)
....collaboration between aerosol/environment scientists & clinicians
Key to all the papers in the thread (& missing from many others)
• • •
Missing some Tweet in this thread? You can try to
force a refresh