
1/
Ever wondered if patients w/ subacromial impingement perform enough strengthening and if adding more will improve outcomes? Our new RCT (n=200) with objective monitoring of exercise dose is out now.
OPENS ACCESS in @AJSM_SportsMed: journals.sagepub.com/doi/full/10.11…
Ever wondered if patients w/ subacromial impingement perform enough strengthening and if adding more will improve outcomes? Our new RCT (n=200) with objective monitoring of exercise dose is out now.
OPENS ACCESS in @AJSM_SportsMed: journals.sagepub.com/doi/full/10.11…
2/
WHY! Well, strengthening exercise is a key component in non-operative care for subacromial impingement, but recent studies suggest that the dose of strengthening exercise is not sufficient in current non-operative care.
WHY! Well, strengthening exercise is a key component in non-operative care for subacromial impingement, but recent studies suggest that the dose of strengthening exercise is not sufficient in current non-operative care.
3/
At this point, it is uncertain if adding more strengthening to current non-operative care is of clinical value.
@DrPeteMalliaras
pubmed.ncbi.nlm.nih.gov/32682937/
At this point, it is uncertain if adding more strengthening to current non-operative care is of clinical value.
@DrPeteMalliaras
pubmed.ncbi.nlm.nih.gov/32682937/
4/
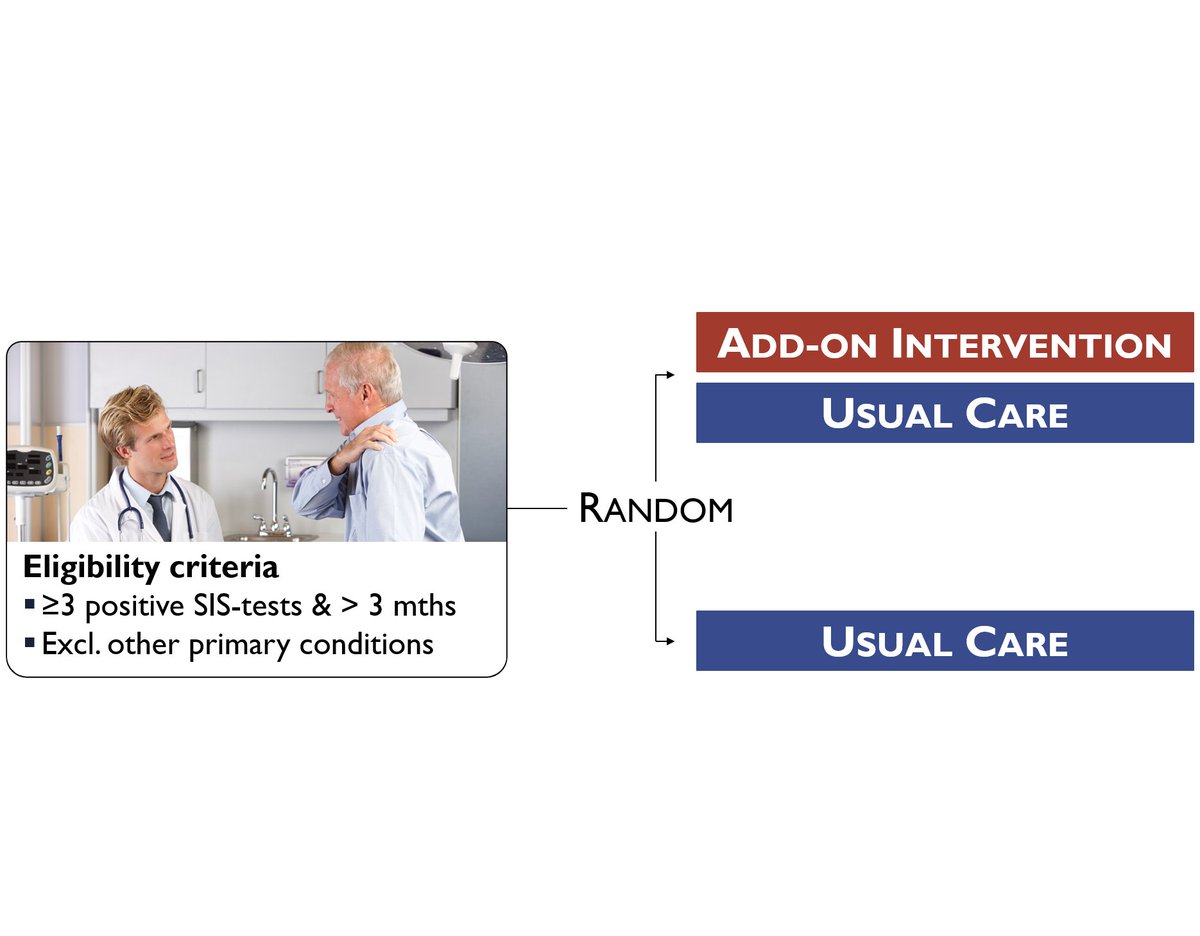
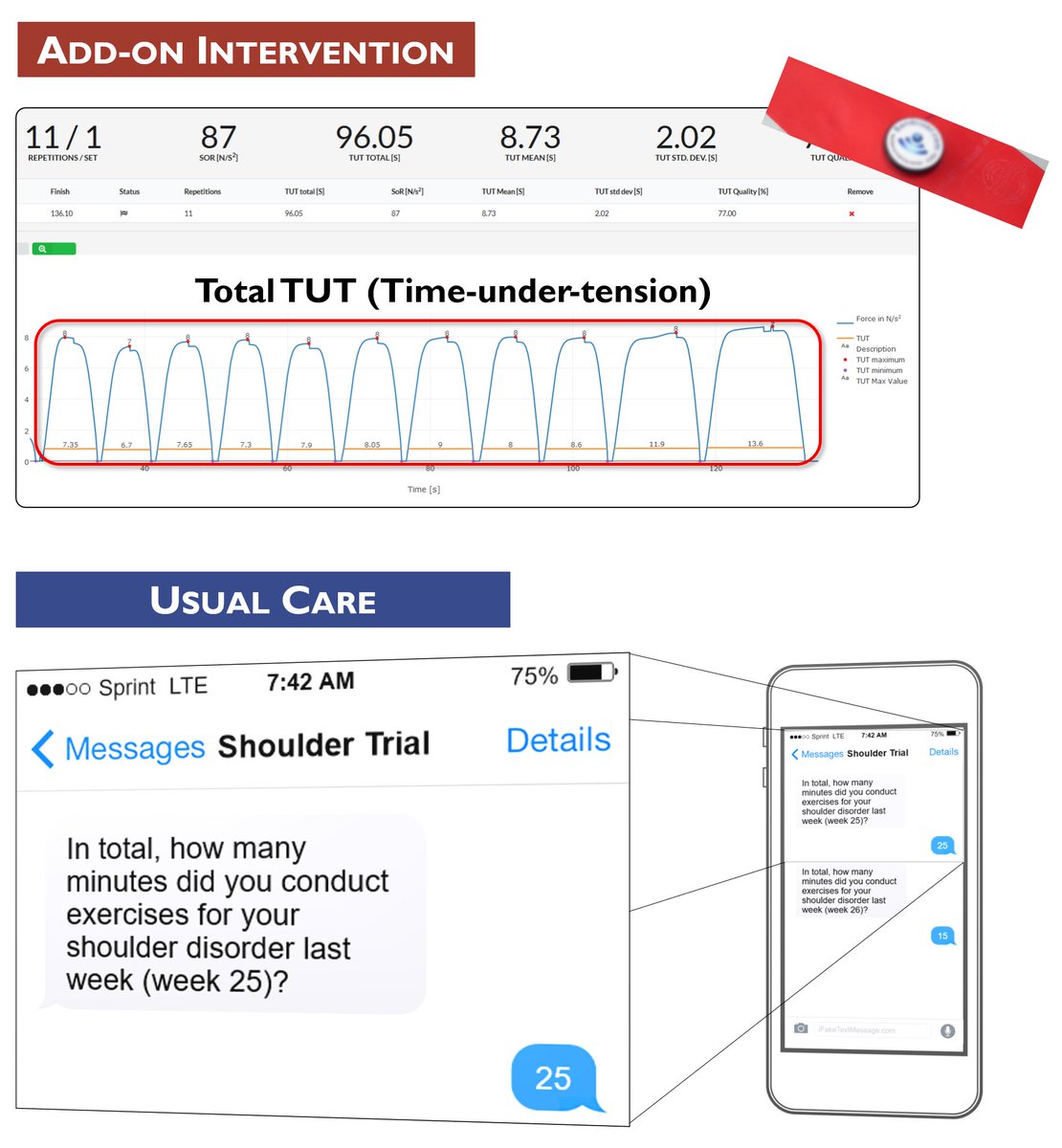
HOW! We screened 89% of ALL the 2047 patients referred to our clinic with ANY shoulder problem. 200 patients were randomized 1:1. Both groups received usual care (referral to free-of-charge PT), the IG also got an add-on intervention.
PROTOCOL: trialsjournal.biomedcentral.com/articles/10.11…
HOW! We screened 89% of ALL the 2047 patients referred to our clinic with ANY shoulder problem. 200 patients were randomized 1:1. Both groups received usual care (referral to free-of-charge PT), the IG also got an add-on intervention.
PROTOCOL: trialsjournal.biomedcentral.com/articles/10.11…
5/
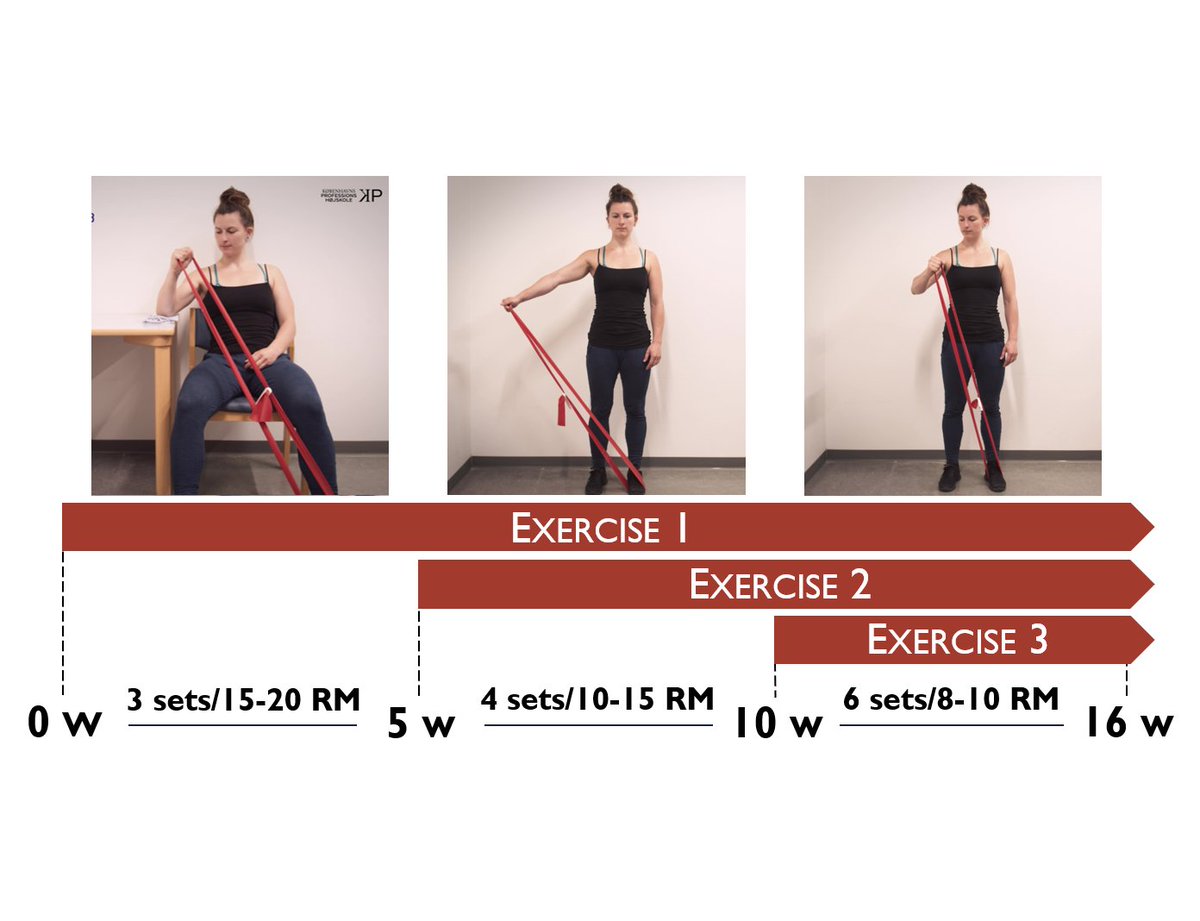
The add-on consisted of three phases of 5-6 weeks each. For each new phase, one exercise was added, and the exercise load increased. All exercises targeted the rotator-cuff muscles and were continued to contraction failure to facilitate an optimised physiological response.
The add-on consisted of three phases of 5-6 weeks each. For each new phase, one exercise was added, and the exercise load increased. All exercises targeted the rotator-cuff muscles and were continued to contraction failure to facilitate an optimised physiological response.
6/
Exercises were performed w slow dynamic contractions and a 5 sec isometric component to increase time-under-tension which is related to greater sub-acute muscle protein synthesis and larger muscle strength gains.
VIDEOS: bit.ly/3oX8KIw
Exercises were performed w slow dynamic contractions and a 5 sec isometric component to increase time-under-tension which is related to greater sub-acute muscle protein synthesis and larger muscle strength gains.
VIDEOS: bit.ly/3oX8KIw
7/
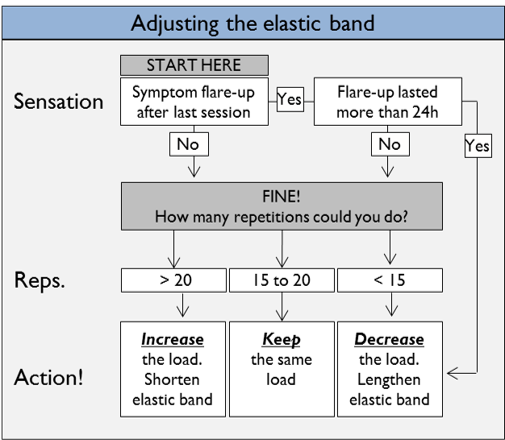
As part of the intervention, we included a standard protocol for individualized adaptation of the exercise load based on pain response and the maximum number of repetitions.
As part of the intervention, we included a standard protocol for individualized adaptation of the exercise load based on pain response and the maximum number of repetitions.
8/
We objectively monitored the actual exercise dose using a sensor mounted on the elastic band and monitored time spent on exercise in usual care through weekly text-messages.
We objectively monitored the actual exercise dose using a sensor mounted on the elastic band and monitored time spent on exercise in usual care through weekly text-messages.
9/
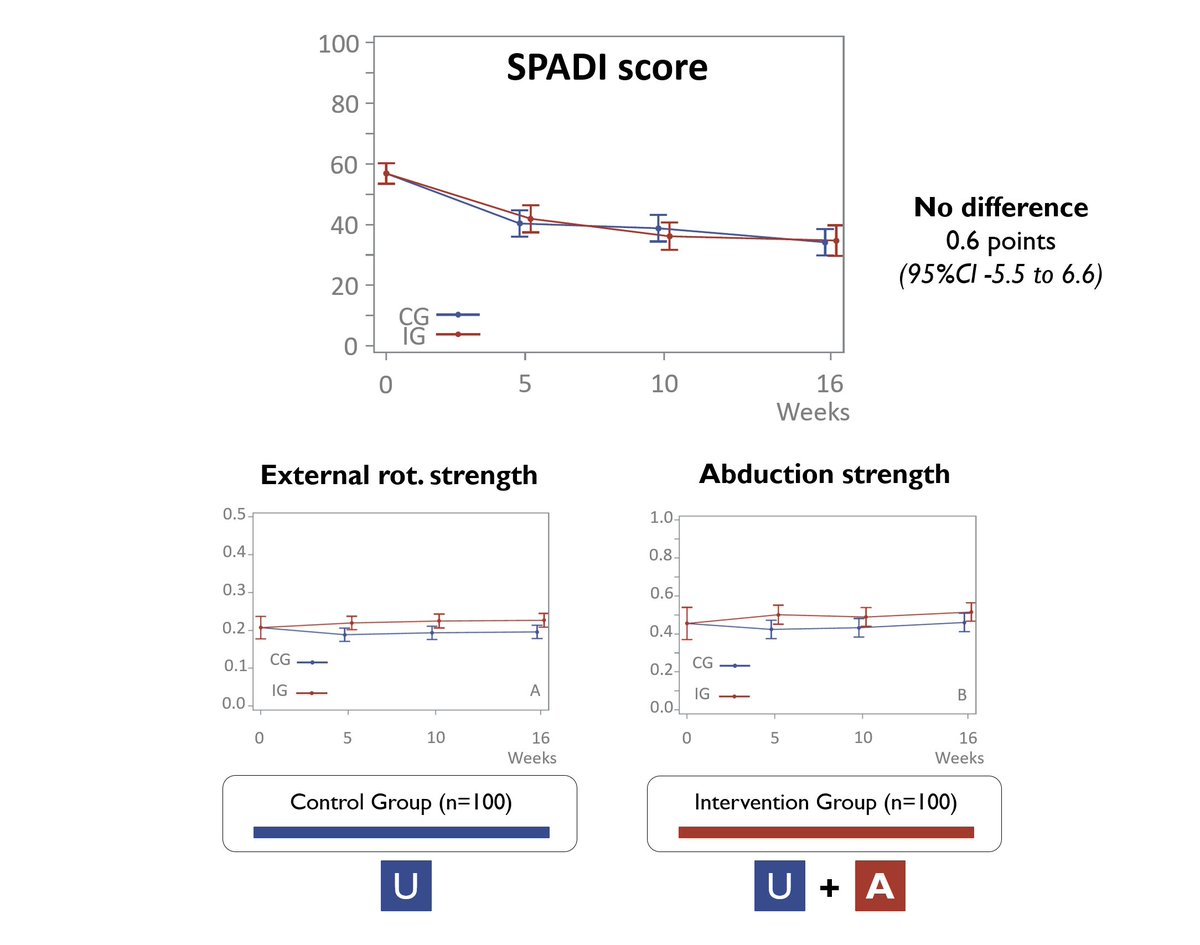
RESULTS: Despite the prescription of a large additional exercise dose, we found NO difference between groups. Not in patient-reported disability (SPADI), nor in strength, ROM or QoL.
Confidence limits for SPADI did not surpass the margin of clinical relevance (10 pts).
RESULTS: Despite the prescription of a large additional exercise dose, we found NO difference between groups. Not in patient-reported disability (SPADI), nor in strength, ROM or QoL.
Confidence limits for SPADI did not surpass the margin of clinical relevance (10 pts).
10/
Time spent on usual care exercise differed between groups. Adjusting did not change results, showing that these would not be different if patients had spent an equal amount of time on usual care exercise.
Also indicates that pts were not able/willing to increase exerc. dose
Time spent on usual care exercise differed between groups. Adjusting did not change results, showing that these would not be different if patients had spent an equal amount of time on usual care exercise.
Also indicates that pts were not able/willing to increase exerc. dose
11/
IN SUMMARY – Adding more does NOT improve outcomes.
But does strengthening exercise still have a part to play in non-op. care for subacromial impingement? Pre-planned secondary studies will shed more light on this topic as well as the importance of central pain adaptations.
IN SUMMARY – Adding more does NOT improve outcomes.
But does strengthening exercise still have a part to play in non-op. care for subacromial impingement? Pre-planned secondary studies will shed more light on this topic as well as the importance of central pain adaptations.
12/
Acknowledgements – This work represents a huge effort from a great research team, all personnel at the department and all the participating patients.
@KThorborg @PerHolmich @MichaelRathleff @TBandholm @SORC_C
Acknowledgements – This work represents a huge effort from a great research team, all personnel at the department and all the participating patients.
@KThorborg @PerHolmich @MichaelRathleff @TBandholm @SORC_C
• • •
Missing some Tweet in this thread? You can try to
force a refresh



